

Predictors of acute toxicities during definitive chemoradiation using intensity-modulated radiotherapy for anal squamous cell carcinoma
- PMID: 25984929
- PMCID: PMC4822488
- DOI: 10.3109/0284186X.2015.1043396
Predictors of acute toxicities during definitive chemoradiation using intensity-modulated radiotherapy for anal squamous cell carcinoma
Abstract
Purpose: To identify clinical and dosimetric factors associated with acute hematologic and gastrointestinal (GI) toxicities during definitive therapy using intensity-modulated radiotherapy (IMRT) for anal squamous cell carcinoma (ASCC).
Materials and methods: We retrospectively analyzed 108 ASCC patients treated with IMRT. Clinical information included age, gender, stage, concurrent chemotherapy, mitomycin (MMC) chemotherapy and weekly hematologic and GI toxicity during IMRT. From contours of the bony pelvis and bowel, dose-volume parameters were extracted. Logistic regression models were used to test associations between toxicities and clinical or dosimetric predictors.
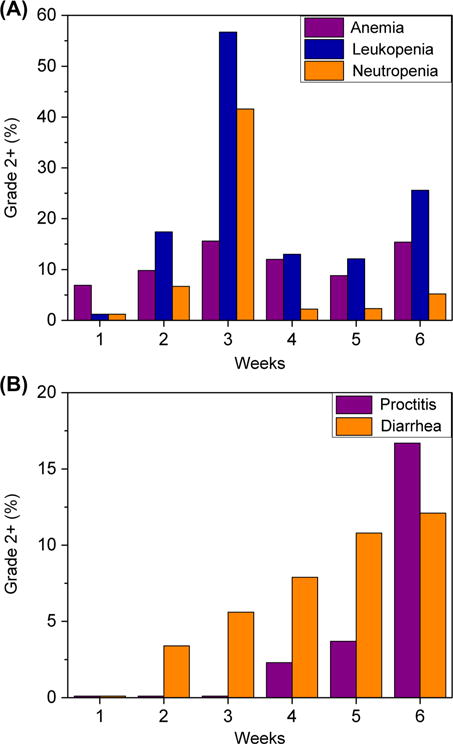
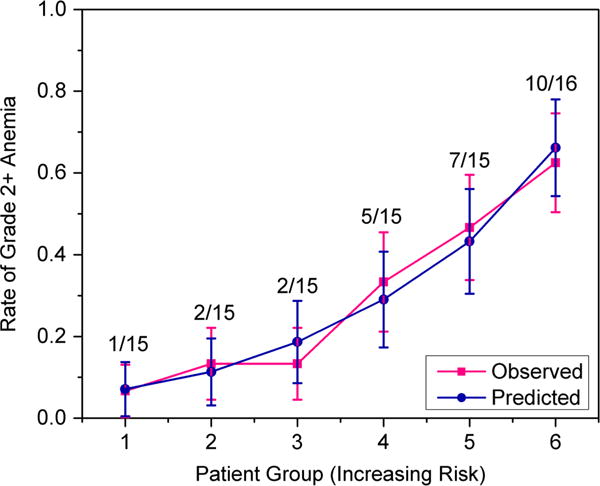
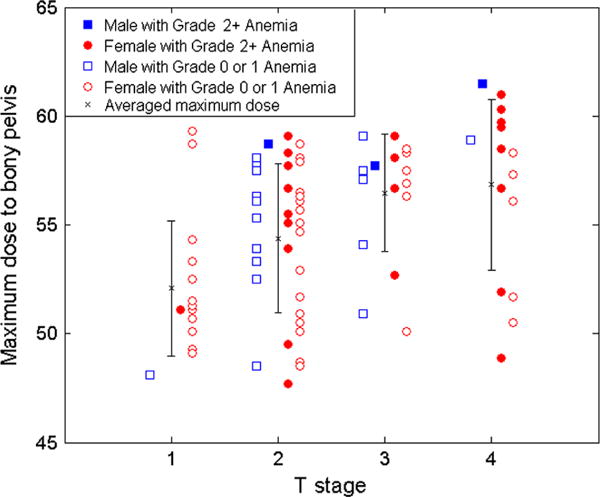
Results: The median age was 59 years, 81 patients were women and 84 patients received concurrent MMC and 5-fluorouracil (5FU). On multivariate analysis (MVA), the model most predictive of Grade 2 + anemia included the maximum bony pelvis dose (Dmax), female gender, and T stage [p = 0.035, cross validation area under the curve (cvAUC) = 0.66]. The strongest model of Grade 2 + leukopenia included V10 (percentage of pelvic bone volume receiving ≥ 10 Gy) and number of MMC cycles (p = 0.276, cvAUC = 0.57). The model including MMC cycle number and T stage correlated best with Grade 2 + neutropenia (p = 0.306, cvAUC = 0.57). The model predictive of combined Grade 2 + hematologic toxicity (HT) included V10 and T stage (p = 0.016, cvAUC = 0.66). A model including VA45 (absolute bowel volume receiving ≥ 45 Gy) and MOH5 (mean dose to hottest 5% of bowel volume) best predicted diarrhea (p = 0.517, cvAUC = 0.56).
Conclusion: Dosimetric constraints to the pelvic bones should be integrated into IMRT planning to reduce toxicity, potentially reducing treatment interruptions and improving disease outcomes in ASCC. Specifically, our results indicate that Dmax should be confined to ≤ 57 Gy to minimize anemia and that V10 should be restricted to ≤ 87% to reduce incidence of all HT.
Conflict of interest statement
Figures
Similar articles
-
Impact of chemotherapy on normal tissue complication probability models of acute hematologic toxicity in patients receiving pelvic intensity modulated radiation therapy.Int J Radiat Oncol Biol Phys. 2013 Dec 1;87(5):983-91. doi: 10.1016/j.ijrobp.2013.09.017. Epub 2013 Oct 22. Int J Radiat Oncol Biol Phys. 2013. PMID: 24161422
-
Dosimetric parameters predictive of acute gastrointestinal toxicity in patients with anal carcinoma treated with concurrent chemotherapy and intensity-modulated radiation therapy.Oncology. 2013;85(1):1-7. doi: 10.1159/000348387. Epub 2013 Jun 1. Oncology. 2013. PMID: 23736101 Clinical Trial.
-
Normal tissue complication probability modeling of acute hematologic toxicity in patients treated with intensity-modulated radiation therapy for squamous cell carcinoma of the anal canal.Int J Radiat Oncol Biol Phys. 2012 Nov 1;84(3):700-6. doi: 10.1016/j.ijrobp.2011.12.072. Epub 2012 Mar 11. Int J Radiat Oncol Biol Phys. 2012. PMID: 22414279
-
Evolution and Management of Treatment-Related Toxicity in Anal Cancer.Surg Oncol Clin N Am. 2017 Jan;26(1):91-113. doi: 10.1016/j.soc.2016.07.004. Surg Oncol Clin N Am. 2017. PMID: 27889040 Review.
-
Treatment of the Primary Tumor in Anal Canal Cancers.Surg Oncol Clin N Am. 2017 Jan;26(1):73-90. doi: 10.1016/j.soc.2016.07.003. Surg Oncol Clin N Am. 2017. PMID: 27889038 Review.
Cited by
-
Dosimetric predictors and Lyman normal tissue complication probability model of hematological toxicity in cervical cancer patients with treated with pelvic irradiation.Med Phys. 2022 Jan;49(1):756-767. doi: 10.1002/mp.15365. Epub 2021 Dec 10. Med Phys. 2022. PMID: 34800297 Free PMC article.
-
Outcomes after intensity-modulated compared with 3-dimensional conformal radiotherapy with chemotherapy for squamous cell carcinoma of the anal canal.Curr Oncol. 2019 Aug;26(4):e515-e521. doi: 10.3747/co.26.4311. Epub 2019 Aug 1. Curr Oncol. 2019. PMID: 31548820 Free PMC article.
-
Advances in the Management of Anal Cancer.Curr Oncol Rep. 2016 Mar;18(3):20. doi: 10.1007/s11912-016-0503-3. Curr Oncol Rep. 2016. PMID: 26905274 Review.
-
De-Escalation of Therapy for Patients with Early-Stage Squamous Cell Carcinoma of the Anus.Cancers (Basel). 2021 Apr 27;13(9):2099. doi: 10.3390/cancers13092099. Cancers (Basel). 2021. PMID: 33925282 Free PMC article. Review.
-
Lymphocyte-Sparing Radiotherapy: The Rationale for Protecting Lymphocyte-rich Organs When Combining Radiotherapy With Immunotherapy.Semin Radiat Oncol. 2020 Apr;30(2):187-193. doi: 10.1016/j.semradonc.2019.12.003. Semin Radiat Oncol. 2020. PMID: 32381298 Free PMC article. Review.
References
-
- Ajani JA, Winter KA, Gunderson LL, Pederson J, Benson AB, 3rd, Thomas CR, Jr, et al. Fluorouracil, mitomycin and radiotherapy vs. fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: A randomized controlled trial. JAMA. 2008;299:1914–21. - PubMed
-
- Bazan JG, Luxton G, Mok EC, Koong AC, Chang DT. Normal tissue complication probability modeling of acute hematologic toxicity in patients treated with intensity modulated radiation therapy for squamous cell carcinoma of the anal canal. Int J Radiat Oncol Biol Phys. 2012;84:700–6. - PubMed
-
- Salama JK, Mell LK, Schomas DA, Miller RC, Devisetty K, Jani AB, et al. Concurrent chemotherapy and intensity-modulated radiation therapy for anal cancer patients: A multicenter experience. J Clin Oncol. 2007;25:4581–6. - PubMed
-
- Saarilahti K, Arponen P, Vaalavirta L, Tenhunen M. The effect of intensity-modulated radiotherapy and high dose rate brachytherapy on acute and late radiotherapy-related adverse events following chemoradiotherapy of anal cancer. Radiother Oncol. 2008;87:383–90. - PubMed
-
- Kachnic LA, Winter K, Myerson RJ, Goodyear MD, Willins J, Esthappan J, et al. RTOG 0529: A phase II evaluation of dose-painted intensity modulated radiation therapy in combination with 5-fluorouracil and mitomycin-C for the reduction of acute morbidity in carcinoma of the anal canal. Int J Radiat Oncol Biol Phys. 2013;86:27–33. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical