

Mortality from cardiovascular diseases in sub-Saharan Africa, 1990-2013: a systematic analysis of data from the Global Burden of Disease Study 2013
- PMID: 25962950
- PMCID: PMC4557490
- DOI: 10.5830/CVJA-2015-036
Mortality from cardiovascular diseases in sub-Saharan Africa, 1990-2013: a systematic analysis of data from the Global Burden of Disease Study 2013
Abstract
Background: Cardiovascular disease (CVD) has been the leading cause of death in developed countries for most of the last century. Most CVD deaths, however, occur in low- and middle-income, developing countries (LMICs) and there is great concern that CVD mortality and burden are rapidly increasing in LMICs as a result of population growth, ageing and health transitions. In sub-Saharan Africa (SSA), where all countries are part of the LMICs, the pattern, magnitude and trends in CVD deaths remain incompletely understood, which limits formulation of data-driven regional and national health policies.
Objective: The aim was to estimate the number of deaths, death rates, and their trends for CVD causes of death in SSA, by age and gender for 1990 and 2013.
Methods: Age- and gender-specific mortality rates for CVD were estimated using the Global Burden of Disease (GBD) 2010 methods with some refinements made by the GBD 2013 study to improve accuracy. Cause of death was estimated as in the GBD 2010 study and updated with a verbal autopsy literature review and cause of death ensemble modelling (CODEm) estimation for causes with sufficient information. For all quantities reported, 95% uncertainty intervals (UIs) were also computed.
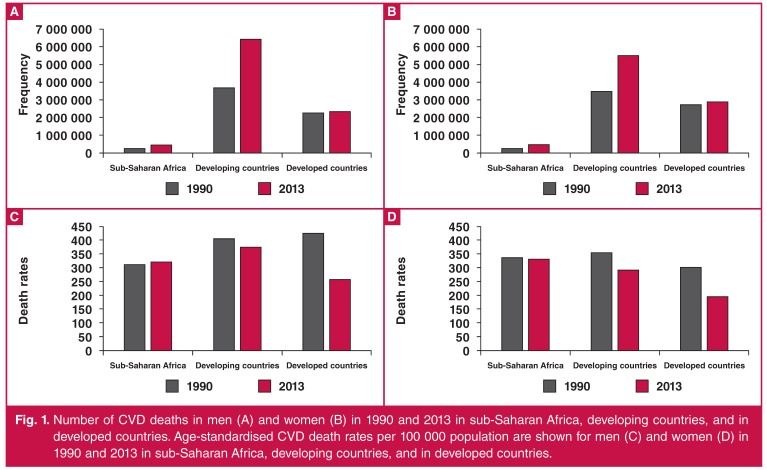
Results: In 2013, CVD caused nearly one million deaths in SSA, constituting 38.3% of non-communicable disease deaths and 11.3% of deaths from all causes in that region. SSA contributed 5.5% of global CVD deaths. There were more deaths in women (512,269) than in men (445,445) and more deaths from stroke (409,840) than ischaemic heart disease (258,939). Compared to 1990, the number of CVD deaths in SSA increased 81% in 2013. Deaths for all component CVDs also increased, ranging from a 7% increase in incidence of rheumatic heart disease to a 196% increase in atrial fibrillation. The age-standardised mortality rate (per 100,000) in 1990 was 327.6 (CI: 306.2-351.7) and 330.2 (CI: 312.9-360.0) in 2013, representing only a 1% increase in more than two decades.
Conclusions: In SSA, CVDs are neither epidemic nor among the leading causes of death. However, a significant increase in the number of deaths from CVDs has occurred since 1990, largely as a result of population growth, ageing and epidemiological transition. Contrary to what has been observed in other world regions, the age-adjusted mortality rate for CVD has not declined. Another important difference in CVD deaths in SSA is the predominance of stroke as the leading cause of death. Attention to aggressive efforts in cardiovascular health promotion and CVD prevention, treatment and control in both men and women are warranted. Additionally, investments to improve directly enumerated epidemiological data for refining the quantitation of risk exposures, death certification and burden of disease assessment will be crucial.
Figures
Similar articles
-
Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013.Lancet. 2015 Jan 10;385(9963):117-71. doi: 10.1016/S0140-6736(14)61682-2. Epub 2014 Dec 18. Lancet. 2015. PMID: 25530442 Free PMC article.
-
Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010.Lancet. 2012 Dec 15;380(9859):2095-128. doi: 10.1016/S0140-6736(12)61728-0. Lancet. 2012. PMID: 23245604 Free PMC article.
-
Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015.Lancet. 2016 Oct 8;388(10053):1459-1544. doi: 10.1016/S0140-6736(16)31012-1. Lancet. 2016. PMID: 27733281 Free PMC article.
-
Cardiovascular Diseases in Sub-Saharan Africa Compared to High-Income Countries: An Epidemiological Perspective.Glob Heart. 2020 Feb 12;15(1):15. doi: 10.5334/gh.403. Glob Heart. 2020. PMID: 32489788 Free PMC article. Review.
-
Burden of cardiovascular disease in Sub-Saharan Africa, 1990-2019: An analysis of the Global Burden of Disease Study.Curr Probl Cardiol. 2024 Jun;49(6):102557. doi: 10.1016/j.cpcardiol.2024.102557. Epub 2024 Mar 29. Curr Probl Cardiol. 2024. PMID: 38554891 Review.
Cited by
-
Factors influencing the implementation of cardiovascular risk scoring in primary care: a mixed-method systematic review.Implement Sci. 2020 Jul 20;15(1):57. doi: 10.1186/s13012-020-01022-x. Implement Sci. 2020. PMID: 32690051 Free PMC article.
-
Prevalence of modifiable cardiovascular risk factors among undergraduate students in Kano Nigeria: A need for action.J Taibah Univ Med Sci. 2021 Dec 3;17(4):578-586. doi: 10.1016/j.jtumed.2021.10.013. eCollection 2022 Aug. J Taibah Univ Med Sci. 2021. PMID: 35983436 Free PMC article.
-
Status of cardiac arrhythmia services in Africa in 2018: a PASCAR Sudden Cardiac Death Task Force report.Cardiovasc J Afr. 2018 Mar/Apr;29(2):115-121. doi: 10.5830/CVJA-2018-027. Cardiovasc J Afr. 2018. PMID: 29745966 Free PMC article.
-
Thirty-day outcomes and predictors of mortality following acute myocardial infarction in northern Tanzania: A prospective observational cohort study.Int J Cardiol. 2021 Nov 1;342:23-28. doi: 10.1016/j.ijcard.2021.08.002. Epub 2021 Aug 5. Int J Cardiol. 2021. PMID: 34364908 Free PMC article.
-
The dietary patterns derived by reduced-rank regression in association with Framingham risk score and lower DASH score in Hoveyzeh cohort study.Sci Rep. 2023 Jul 8;13(1):11093. doi: 10.1038/s41598-023-37809-3. Sci Rep. 2023. PMID: 37422506 Free PMC article.
References
-
- et al. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;14:10–6736. - PubMed
-
- et al. National Vital Statistics System HIST290A: Deaths for selected causes by 10-year age groups, race, and sex: Death registration states, 1900–32, and United States, 1933–98. URL: http://www.cdc.gov/nchs/nvss/mortality/hist290a.htm. NCHS/NVSS 15 A.D. January 18. Available at:
-
- Promoting Cardiovascular Health in the Developing World: A Critical Challenge to Achieve Global Health. Washington, DC: National Academies Press; 2010. - PubMed
-
- Preventing the Global Epidemic of Cardiovascular Disease: Meeting the Challenges in Developing Countries. Washington, DC: National Academies Press; 2010.
-
- et al. Prevention and control of non-communicable diseases – Report of the Secretary-General. URL: http://www.un.org/ga/search/view_doc.asp?symbol=A/66/83&Lang=E. World Health Organization. 2011:1–18. Available at:
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials