

ABO-compatible liver allograft antibody-mediated rejection: an update
- PMID: 25944231
- PMCID: PMC4646419
- DOI: 10.1097/MOT.0000000000000194
ABO-compatible liver allograft antibody-mediated rejection: an update
Abstract
Purpose of review: Liver allograft antibody-mediated rejection (AMR) studies have lagged behind parallel efforts in kidney and heart because of a comparative inherent hepatic resistance to AMR. Three developments, however, have increased interest: first, solid phase antibody testing enabled more precise antibody characterization; second, increased expectations for long-term, morbidity-free survival; and third, immunosuppression minimization trials.
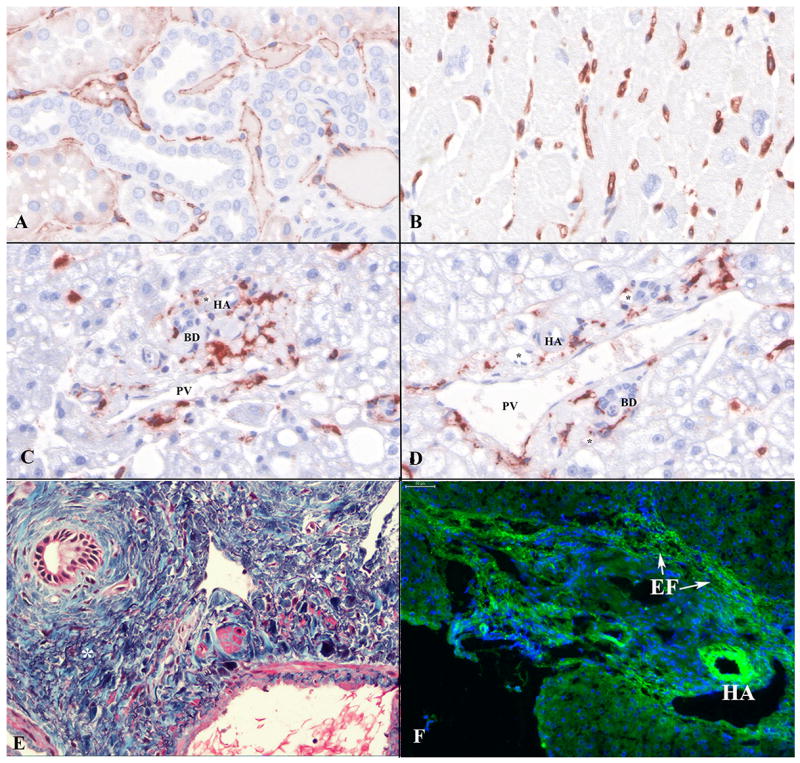
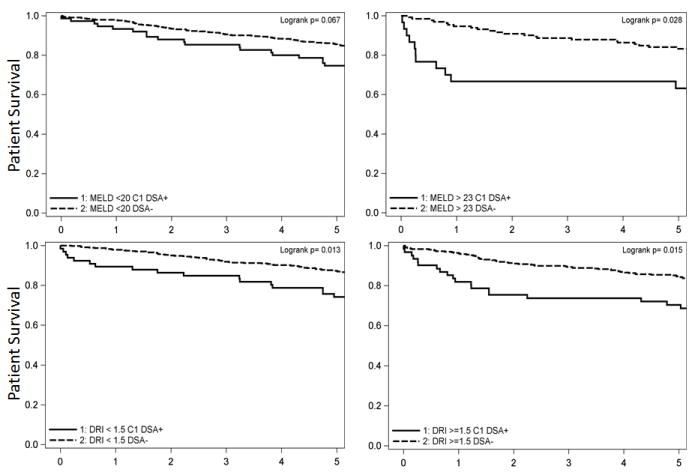
Recent findings: Two overlapping liver allograft AMR phenotypic expressions are beginning to emerge: acute and chronic AMR. Acute AMR usually occurs within the several weeks after transplantation and characterized clinically by donor-specific antibodies (DSA) persistence, allograft dysfunction, thrombocytopenia, and hypocomplementemia. Acute AMR appears histopathologically similar to acute AMR in other organs: diffuse microvascular endothelial cell hypertrophy, C4d deposits, neutrophilic, eosinophilic, and macrophag-mediated microvasculitis/capillaritis, along with liver-specific ductular reaction, centrilobular hepatocyte swelling, and hepatocanalicular cholestasis often combined with T-cell-mediated rejection (TCMR). Chronic AMR is less well defined, but strongly linked to serum class II DSA and associated with late-onset acute TCMR, fibrosis, chronic rejection, and decreased survival. Unlike acute AMR, chronic AMR is a slowly evolving insult with a number of potential manifestations, but most commonly appears as low-grade lymphoplasmacytic portal and perivenular inflammation accompanied by unusual fibrosis patterns and variable microvascular C4d deposition; capillaritis can be more difficult to identify than in acute AMR.
Summary: More precise DSA characterization, increasing expectations for long-term survival, and immunosuppression weaning precipitated a re-emergence of liver allograft AMR interest. Pathophysiological similarities exist between heart, kidney, and liver allografts, but liver-specific considerations may prove critical to our ultimate understanding of all solid organ AMR.
Conflict of interest statement
Conflicts of interest: none
Figures
Similar articles
-
Significance of complement split product C4d in ABO-compatible liver allograft: diagnosing utility in acute antibody mediated rejection.Transpl Immunol. 2012 Jan;26(1):62-9. doi: 10.1016/j.trim.2011.08.005. Epub 2011 Sep 1. Transpl Immunol. 2012. PMID: 21907804
-
Prevention and treatment of liver allograft antibody-mediated rejection and the role of the 'two-hit hypothesis'.Curr Opin Organ Transplant. 2016 Apr;21(2):209-18. doi: 10.1097/MOT.0000000000000275. Curr Opin Organ Transplant. 2016. PMID: 26918881 Review.
-
Acute Antibody-mediated rejection in liver transplantation: Impact and applicability of the Banff working group on liver allograft pathology 2016 criteria.Hum Pathol. 2022 Sep;127:67-77. doi: 10.1016/j.humpath.2022.06.015. Epub 2022 Jun 18. Hum Pathol. 2022. PMID: 35728694
-
Application of complement component 4d immunohistochemistry to ABO-compatible and ABO-incompatible liver transplantation.Liver Transpl. 2014 Feb;20(2):200-9. doi: 10.1002/lt.23789. Liver Transpl. 2014. PMID: 24470446
-
Acute antibody-mediated rejection in ABO-compatible pediatric liver transplant recipients: case series and review of the literature.Pediatr Transplant. 2017 Feb;21(1). doi: 10.1111/petr.12791. Epub 2016 Sep 5. Pediatr Transplant. 2017. PMID: 27597379 Review.
Cited by
-
Environmental peer pressure: CD4+ T cell help in tolerance and transplantation.Liver Transpl. 2018 Jan;24(1):89-97. doi: 10.1002/lt.24873. Liver Transpl. 2018. PMID: 28926189 Free PMC article. Review.
-
The fate of anti-HLA antibodies following liver transplantation.Front Nephrol. 2024 Jun 12;4:1403096. doi: 10.3389/fneph.2024.1403096. eCollection 2024. Front Nephrol. 2024. PMID: 38933742 Free PMC article.
-
The Role of Humoral Alloreactivity in Liver Transplantation: Lessons Learned and New Perspectives.J Immunol Res. 2017;2017:3234906. doi: 10.1155/2017/3234906. Epub 2017 Jan 9. J Immunol Res. 2017. PMID: 28164136 Free PMC article. Review.
-
Antibody-Mediated Rejection in Liver Transplantation: Immuno-Pathological Characteristics and Long-Term Follow-Up.Transpl Int. 2024 Aug 29;37:13232. doi: 10.3389/ti.2024.13232. eCollection 2024. Transpl Int. 2024. PMID: 39267618 Free PMC article.
-
Five-year histological and serological follow-up of operationally tolerant pediatric liver transplant recipients enrolled in WISP-R.Hepatology. 2017 Feb;65(2):647-660. doi: 10.1002/hep.28681. Epub 2016 Jul 27. Hepatology. 2017. PMID: 27302659 Free PMC article. Clinical Trial.
References
-
- Gugenheim J, Amorosa L, Gigou M, Fabiani B, Rouger P, Gane P, Reynes M, Bismuth H. Specific absorption of lymphocytotoxic alloantibodies by the liver in inbred rats. Transplantation. 1990;50:309–313. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
