

Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience
- PMID: 25889427
- PMCID: PMC4382928
- DOI: 10.1186/s13000-015-0233-0
Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience
Abstract
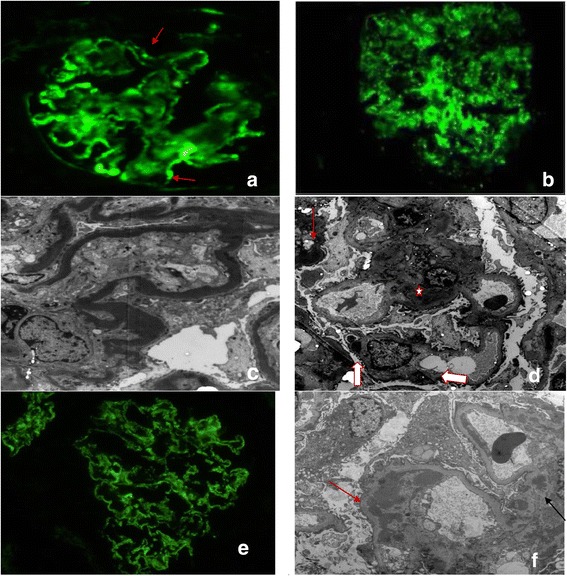
Background: C3 glomerulopathy (C3GP) is characterized by deposition of complement C3 with absence/traces of immunoglobulins in the glomeruli and categorized into dense deposit disease (DDD), C3 glomerulonephritis (C3GN), complement factor H related protein 5(CFHR5) nephropathy etc. Collaborative efforts of pathologists, complement biologists and nephrologists worldwide are expanding the histomorphological pattern and laboratory findings related to C3GP. Hence, we studied point prevalence and morphological spectrum of C3GP in Indian patients to correlate morphological patterns with standard therapies and outcome of the patients.
Methods: Retrospective analysis of renal biopsies (2007-2012,n-4565), which on immunofluorescence (IF) had C3 dominant deposits with absence or trace amount of immunoglobulin was carried out. Histopathology and electronmicroscopy (EM) were reviewed; cases were re-classified as DDD and C3GN. Histomorphological patterns of both groups were compared and correlated with treatment. Clinical details and follow up of patients were retrieved from the department of nephrology.
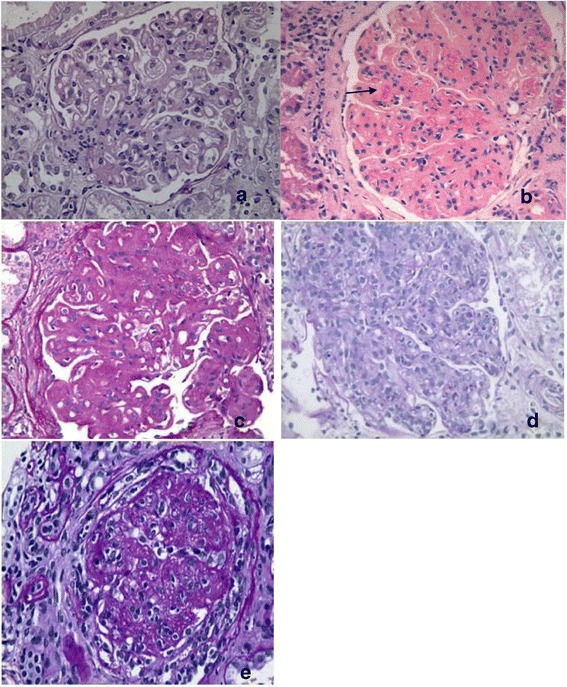
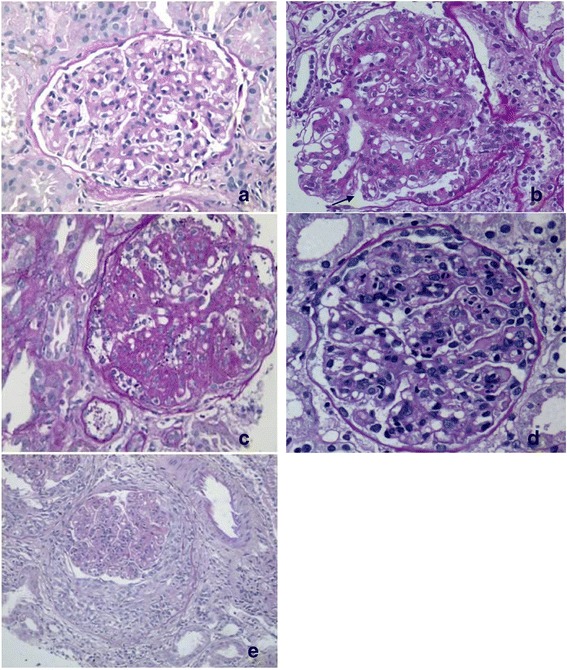
Results: There were 31 cases (0.7%) of C3GP sub-classified as DDD (n-13) and C3GN (n-14). It was difficult to sub-classify 4 cases since EM showed overlapping features. C3GN and DDD had distinct clinical characteristics and disease outcome, though pathological features were overlapping. Majority of C3GP patients were males and were in 2(nd) to 4(th) decade of life. Nephrotic syndrome in DDD and nephritic-nephrotic presentation in C3GN patients was more common. Hypertension and oliguria were more often observed in C3GN than DDD. Membranoproliferative pattern (MPGN) was commonest pattern in DDD; other patterns seen were mesangial proliferative, mesangial expansive/nodular, exudative and crescentic. C3GN also had all the above patterns, the predominant ones being MPGN and mesangial proliferative. Limited follow-up revealed response to therapy only in C3GN (33%). Progression to ESRD was 33% in DDD and 10% cases in C3GN.
Conclusion: C3GP comprise 0.7% of all renal biopsies. MPGN pattern was the commonest morphological pattern in DDD whereas MPGN and mesangial proliferative pattern were equally dominant patterns in C3GN. EM of 4 cases (13%) showed intermediate features. Evaluation of alternate complement pathway must be done in all cases to identify the point of dysregulated alternate complement pathway and to confirm the diagnosis in ambiguous cases.
Virtual slides: The virtual slides for this article can be found here: http://www.diagnosticpathology.diagnomx.eu/vs/1730070964135632.
Figures
Similar articles
-
Membranoproliferative glomerulonephritis and C3 glomerulonephritis: frequency, clinical features, and outcome in children.Nephrology (Carlton). 2015 Apr;20(4):286-92. doi: 10.1111/nep.12382. Nephrology (Carlton). 2015. PMID: 25524631
-
C3 glomerulopathy: clinicopathologic features and predictors of outcome.Clin J Am Soc Nephrol. 2014 Jan;9(1):46-53. doi: 10.2215/CJN.04700513. Epub 2013 Oct 31. Clin J Am Soc Nephrol. 2014. PMID: 24178974 Free PMC article.
-
C3 glomerulonephritis and dense deposit disease share a similar disease course in a large United States cohort of patients with C3 glomerulopathy.Kidney Int. 2018 Apr;93(4):977-985. doi: 10.1016/j.kint.2017.10.022. Epub 2018 Jan 6. Kidney Int. 2018. PMID: 29310824
-
C3 glomerulopathy.Contrib Nephrol. 2013;181:185-93. doi: 10.1159/000348654. Epub 2013 May 8. Contrib Nephrol. 2013. PMID: 23689580 Review.
-
C3 glomerulopathy and current dilemmas.Clin Exp Nephrol. 2017 Aug;21(4):541-551. doi: 10.1007/s10157-016-1358-5. Epub 2016 Nov 23. Clin Exp Nephrol. 2017. PMID: 27878657 Free PMC article. Review.
Cited by
-
Poor allograft outcome in Indian patients with post-transplant C3 glomerulopathy.Clin Kidney J. 2019 Nov 4;14(1):291-300. doi: 10.1093/ckj/sfz135. eCollection 2021 Jan. Clin Kidney J. 2019. PMID: 33564431 Free PMC article.
-
Long-term follow-up including extensive complement analysis of a pediatric C3 glomerulopathy cohort.Pediatr Nephrol. 2022 Mar;37(3):601-612. doi: 10.1007/s00467-021-05221-6. Epub 2021 Sep 2. Pediatr Nephrol. 2022. PMID: 34476601 Free PMC article.
-
Dense deposit disease: a greatly increased biopsy incidence in India versus the USA.Clin Kidney J. 2019 Jan 8;12(4):476-482. doi: 10.1093/ckj/sfy125. eCollection 2019 Aug. Clin Kidney J. 2019. PMID: 31384437 Free PMC article.
-
Usefulness of mycophenolate mofetil in Indian patients with C3 glomerulopathy.Clin Kidney J. 2018 Dec 24;12(4):483-487. doi: 10.1093/ckj/sfy127. eCollection 2019 Aug. Clin Kidney J. 2018. PMID: 31384438 Free PMC article.
-
Renal Tubular Complement 3 Deposition in Children with Primary Nephrotic Syndrome.Biomed Res Int. 2018 May 30;2018:4386438. doi: 10.1155/2018/4386438. eCollection 2018. Biomed Res Int. 2018. PMID: 30003098 Free PMC article.
References
-
- Jackson E, McAdams A, Strife C, Forristal J, Welch T, West C. Differences between membranoproliferative glomerulonephritis types I and III in clinical presentation, glomerular morphology, and complement perturbation. Am J Kidney Dis. 1987;9(2):115–20. doi: 10.1016/S0272-6386(87)80088-4. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
