

Identification of viral and bacterial pathogens from hospitalized children with severe acute respiratory illness in Lusaka, Zambia, 2011-2012: a cross-sectional study
- PMID: 25888024
- PMCID: PMC4391483
- DOI: 10.1186/s12879-015-0779-1
Identification of viral and bacterial pathogens from hospitalized children with severe acute respiratory illness in Lusaka, Zambia, 2011-2012: a cross-sectional study
Abstract
Background: Morbidity and mortality from respiratory infections are higher in resource-limited countries than developed countries, but limited studies have been conducted in resource-limited settings to examine pathogens from patients with acute respiratory infections. Influenza surveillance has been conducted in Zambia since 2008; however, only 4.3% of patients enrolled in 2011-2012 were positive for influenza. Therefore, we examined non-influenza respiratory pathogens in children with severe acute respiratory illness (SARI) in Zambia, to estimate the scope of disease burden and determine commonly-identified respiratory pathogens.
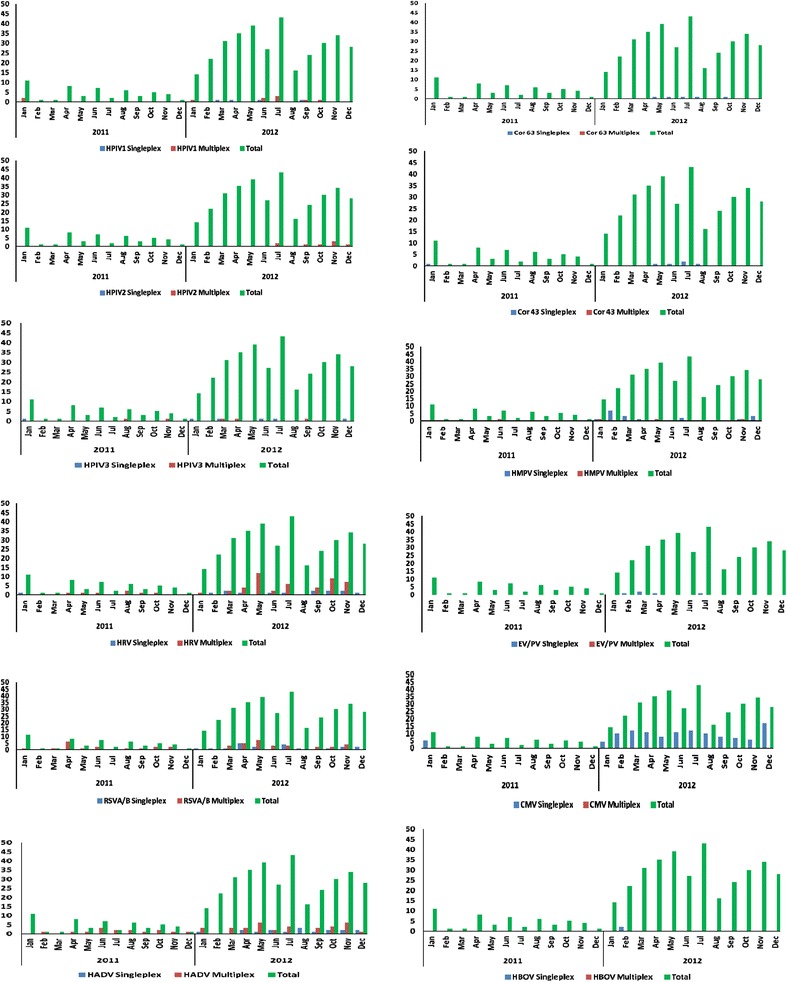
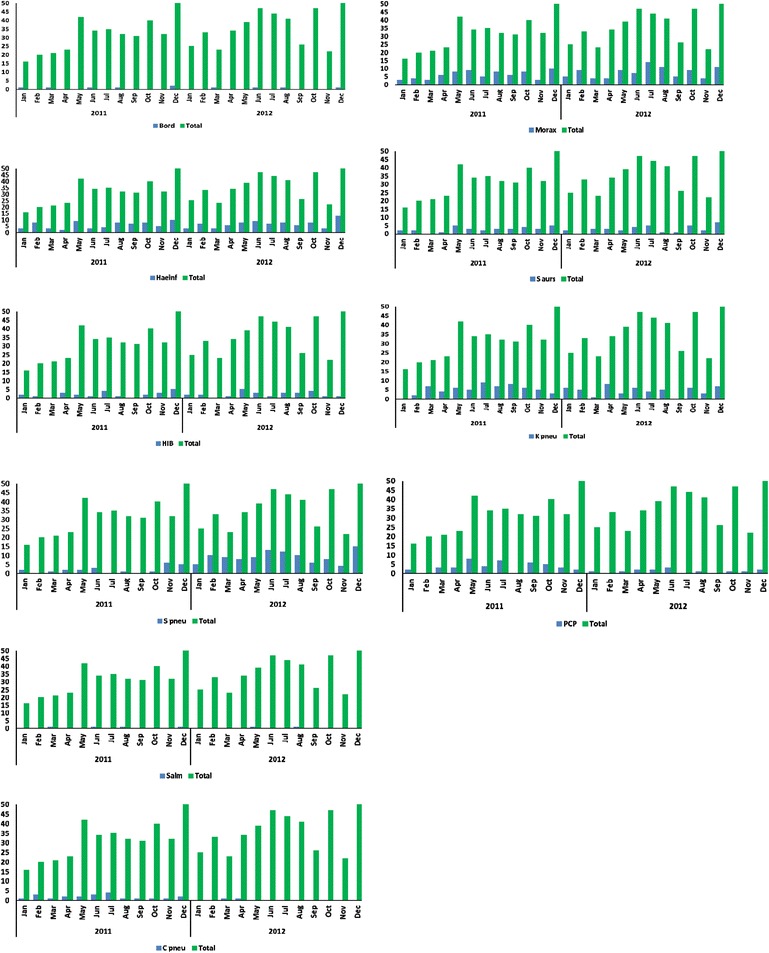
Methods: Two reverse transcriptase polymerase chain reaction (rRT-PCR) methods (single and multiplex) were used to analyze nasopharyngeal and throat swabs collected from SARI cases under five years of age from January 2011 through December 2012. All specimens were negative for influenza by rRT-PCR. The panel of singleplex reactions targeted seven viruses, while the multiplex assay targeted thirty-three bacteria, fungi, and viruses.
Results: A set of 297 specimens were tested by singleplex rRT-PCR, and a different set of 199 were tested by multiplex rRT-PCR. Using the singleplex assay, 184/297 (61.9%) specimens were positive for one or more viruses. The most prevalent viruses were human rhinovirus (57/297; 19.2%), human adenovirus (50/297; 16.8%), and respiratory syncytial virus (RSV) (45/297; 15.2%). Using multiplex PCR, at least one virus was detected from 167/199 (83.9%) specimens, and at least one bacteria was detected from 197/199 (99.0%) specimens. Cytomegalovirus (415/199; 208.5%) and RSV (67/199; 33.7%) were the most commonly detected viruses, while Streptococcus pneumonie (109/199; 54.8%) and Moraxella catarrhalis (92/199; 46.2%) were the most commonly detected bacteria.
Conclusions: Single infections and co-infections of many viruses and bacteria were identified in children with SARI. These results provide an estimate of the prevalence of infection and show which respiratory pathogens are commonly identified in patients. Further studies should investigate causal associations between individual pathogens and SARI.
Figures
Similar articles
-
Epidemiological and etiological characteristics of 1266 patients with severe acute respiratory infection in central China, 2018-2020: a retrospective survey.BMC Infect Dis. 2024 Apr 22;24(1):426. doi: 10.1186/s12879-024-09297-x. BMC Infect Dis. 2024. PMID: 38649799 Free PMC article.
-
Viral and Atypical Bacterial Detection in Young Nepalese Children Hospitalized with Severe Pneumonia.Microbiol Spectr. 2021 Oct 31;9(2):e0055121. doi: 10.1128/Spectrum.00551-21. Epub 2021 Oct 27. Microbiol Spectr. 2021. PMID: 34704788 Free PMC article.
-
Respiratory viral coinfections identified by a 10-plex real-time reverse-transcription polymerase chain reaction assay in patients hospitalized with severe acute respiratory illness--South Africa, 2009-2010.J Infect Dis. 2012 Dec 15;206 Suppl 1:S159-65. doi: 10.1093/infdis/jis538. J Infect Dis. 2012. PMID: 23169964
-
The role of multiplex PCR in respiratory tract infections in children.Dtsch Arztebl Int. 2014 Sep 19;111(38):639-45. doi: 10.3238/arztebl.2014.0639. Dtsch Arztebl Int. 2014. PMID: 25316519 Free PMC article. Review.
-
Lethal synergistic infections by two concurrent respiratory pathogens.Arch Med Res. 2024 Oct 24;56(1):103101. doi: 10.1016/j.arcmed.2024.103101. Online ahead of print. Arch Med Res. 2024. PMID: 39454459 Review.
Cited by
-
Performance comparison of three commercial multiplex molecular panels for respiratory viruses at a South African academic hospital.Afr J Lab Med. 2024 Aug 20;13(1):2415. doi: 10.4102/ajlm.v13i1.2415. eCollection 2024. Afr J Lab Med. 2024. PMID: 39228900 Free PMC article.
-
Contemporaneous data on the prevalence of Human Respiratory Syncytial Virus infection in people with acute respiratory tract infections in Africa (2000-2017).Data Brief. 2018 Aug 22;20:940-947. doi: 10.1016/j.dib.2018.08.039. eCollection 2018 Oct. Data Brief. 2018. PMID: 30225305 Free PMC article.
-
Postviral Complications: Bacterial Pneumonia.Clin Chest Med. 2017 Mar;38(1):127-138. doi: 10.1016/j.ccm.2016.11.006. Epub 2016 Dec 13. Clin Chest Med. 2017. PMID: 28159155 Free PMC article. Review.
-
Multicenter study to describe viral etiologies, clinical profiles, and outcomes of hospitalized children with severe acute respiratory infections, Egypt 2022.Sci Rep. 2023 Dec 9;13(1):21860. doi: 10.1038/s41598-023-48814-x. Sci Rep. 2023. PMID: 38071208 Free PMC article.
-
Prevalence of human respiratory syncytial virus infection in people with acute respiratory tract infections in Africa: A systematic review and meta-analysis.Influenza Other Respir Viruses. 2018 Nov;12(6):793-803. doi: 10.1111/irv.12584. Epub 2018 Jul 5. Influenza Other Respir Viruses. 2018. PMID: 29908103 Free PMC article.
References
-
- World Health Organization: World Health Report 2008 Statistical Anne. Genève: http://www.who.int/whosis/whostat/EN_WHS2011_Full.pdf?ua=1
-
- World Health Organization: Acute respiratory infections in children. http://www.who.int/pmnch/media/press_materials/fs/fs_mdg4_childmortality....
-
- Iwane MK, Edwards KM, Szilagyi PG, Walker FJ, Griffin MR, Weinberg GA, et al. Population–based surveillance for hospitalizations associated with respiratory syncytial virus, influenza virus and parainfluenza viruses among young children. J Pediatr. 2004;10:113–1758. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
