

Dynamic changes of microbial flora and therapeutic consequences in persistent peritonitis
- PMID: 25887649
- PMCID: PMC4354758
- DOI: 10.1186/s13054-015-0789-9
Dynamic changes of microbial flora and therapeutic consequences in persistent peritonitis
Abstract
Introduction: Persistent peritonitis is a frequent complication of secondary peritonitis requiring additional reoperations and antibiotic therapy. This situation raises specific concerns due to microbiological changes in peritoneal samples, especially the emergence of multidrug-resistant (MDR) strains. Although this complication has been extensively studied, the rate and dynamics of MDR strains have rarely been analysed.
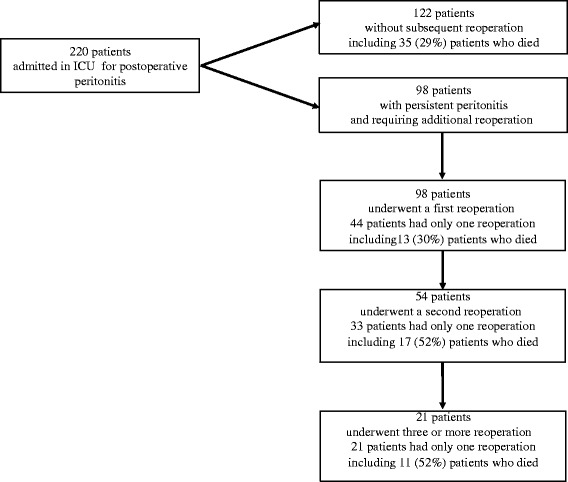
Methods: We compared the clinical, microbiological and therapeutic data of consecutive ICU patients admitted for postoperative peritonitis either without subsequent reoperation (n = 122) or who underwent repeated surgery for persistent peritonitis with positive peritoneal fluid cultures (n = 98). Data collected on index surgery for the treatment of postoperative peritonitis were compared between these two groups. In the patients with persistent peritonitis, the data obtained at the first, second and third reoperations were compared with those of index surgery. Risk factors for emergence of MDR strains were assessed.
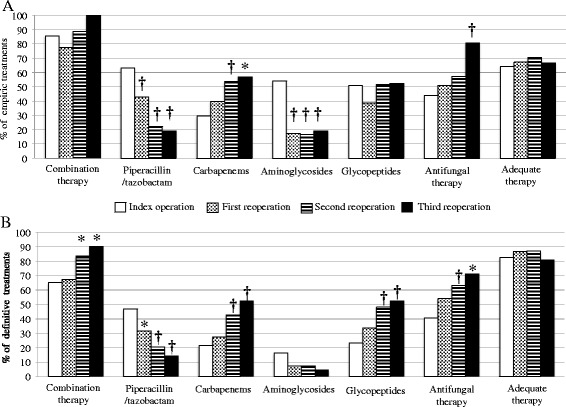
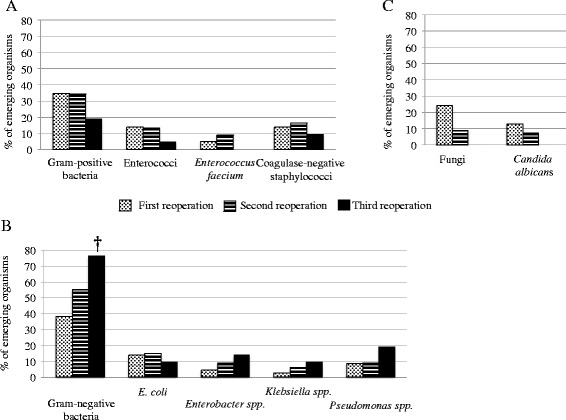
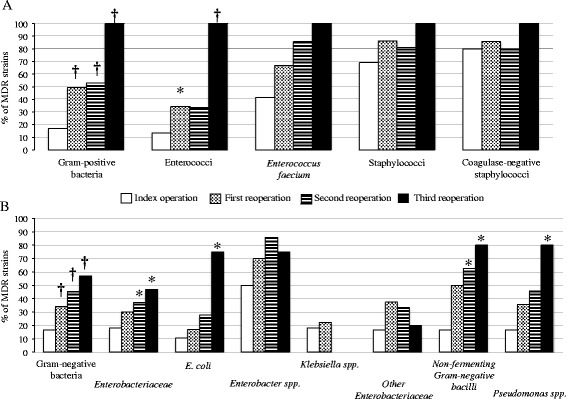
Results: At the time of index surgery, no parameters were able to differentiate patients with or without persistent peritonitis except for increased severity and high proportions of fungal isolates in the persistent peritonitis group. The mean time to reoperation was similar from the first to the third reoperation (range: 5 to 6 days). Septic shock was the main clinical expression of persistent peritonitis. A progressive shift of peritoneal flora was observed with the number of reoperations, comprising extinction of susceptible strains and emergence of 85 MDR strains. The proportion of patients harbouring MDR strains increased from 41% at index surgery, to 49% at the first, 54% at the second (P = 0.037) and 76% at the third reoperation (P = 0.003 versus index surgery). In multivariate analysis, the only risk factor for emergence of MDR strains was time to reoperation (OR 1.19 per day, 95%CI (1.08 to 1.33), P = 0.0006).
Conclusions: Initial severity, presence of Candida in surgical samples and inadequate source control are the major risk factors for persistent peritonitis. Emergence of MDR bacteria is frequent and increases progressively with the number of reoperations. No link was demonstrated between emergence of MDR strains and antibiotic regimens, while source control and its timing appeared to be major determinants of emergence of MDR strains.
Figures
Similar articles
-
Positive peritoneal fluid fungal cultures in postoperative peritonitis after bariatric surgery.Clin Microbiol Infect. 2015 Sep;21(9):853.e1-3. doi: 10.1016/j.cmi.2015.05.024. Epub 2015 May 29. Clin Microbiol Infect. 2015. PMID: 26033667
-
Understanding the acute inflammatory response to Pseudomonas aeruginosa infection: differences between susceptible and multidrug-resistant strains in a mouse peritonitis model.Int J Antimicrob Agents. 2017 Feb;49(2):198-203. doi: 10.1016/j.ijantimicag.2016.10.016. Epub 2016 Nov 28. Int J Antimicrob Agents. 2017. PMID: 27939091
-
Risk factors for multidrug resistant bacteria and optimization of empirical antibiotic therapy in postoperative peritonitis.Crit Care. 2010;14(1):R20. doi: 10.1186/cc8877. Epub 2010 Feb 15. Crit Care. 2010. PMID: 20156360 Free PMC article.
-
[Characteristics of postoperative peritonitis].Chirurg. 2016 Jan;87(1):20-5. doi: 10.1007/s00104-015-0110-0. Chirurg. 2016. PMID: 26541449 Review. German.
-
[Candida peritonitis].Enferm Infecc Microbiol Clin. 2010 Sep;28 Suppl 2:42-8. doi: 10.1016/S0213-005X(10)70029-X. Enferm Infecc Microbiol Clin. 2010. PMID: 21130929 Review. Spanish.
Cited by
-
Post-operative abdominal infections: epidemiology, operational definitions, and outcomes.Intensive Care Med. 2020 Feb;46(2):163-172. doi: 10.1007/s00134-019-05841-5. Epub 2019 Nov 7. Intensive Care Med. 2020. PMID: 31701205 Review.
-
Microbiological profile of patients treated for postoperative peritonitis: temporal trends 1999-2019.World J Emerg Surg. 2023 Dec 19;18(1):58. doi: 10.1186/s13017-023-00528-1. World J Emerg Surg. 2023. PMID: 38115142 Free PMC article.
-
Management of intra-abdominal infections: recommendations by the WSES 2016 consensus conference.World J Emerg Surg. 2017 May 4;12:22. doi: 10.1186/s13017-017-0132-7. eCollection 2017. World J Emerg Surg. 2017. PMID: 28484510 Free PMC article. Review.
-
Characteristics and outcomes of anti-infective de-escalation during health care-associated intra-abdominal infections.Crit Care. 2016 Apr 7;20:83. doi: 10.1186/s13054-016-1267-8. Crit Care. 2016. PMID: 27052675 Free PMC article.
-
Short-course antibiotic therapy for critically ill patients treated for postoperative intra-abdominal infection: the DURAPOP randomised clinical trial.Intensive Care Med. 2018 Mar;44(3):300-310. doi: 10.1007/s00134-018-5088-x. Epub 2018 Feb 26. Intensive Care Med. 2018. PMID: 29484469 Clinical Trial.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
