

Renal function interferes with copeptin in prediction of major adverse cardiac events in patients undergoing vascular surgery
- PMID: 25875814
- PMCID: PMC4395325
- DOI: 10.1371/journal.pone.0123093
Renal function interferes with copeptin in prediction of major adverse cardiac events in patients undergoing vascular surgery
Abstract
Objective: Precise perioperative risk stratification is important in vascular surgery patients who are at high risk for major adverse cardiovascular events (MACE) peri- and postoperatively. In clinical practice, the patient's perioperative risk is predicted by various indicators, e.g. revised cardiac index (RCRI) or modifications thereof. Patients suffering from chronic kidney disease (CKD) are stratified into a higher risk category. We hypothesized that Copeptin as a novel biomarker for hemodynamic stress could help to improve the prediction of perioperative cardiovascular events in patients undergoing vascular surgery including patients with chronic kidney disease.
Methods: 477 consecutive patients undergoing abdominal aortic, peripheral arterial or carotid surgery from June 2007 to October 2012 were prospectively enrolled. Primary endpoint was 30-day postoperative major adverse cardiovascular events (MACE).
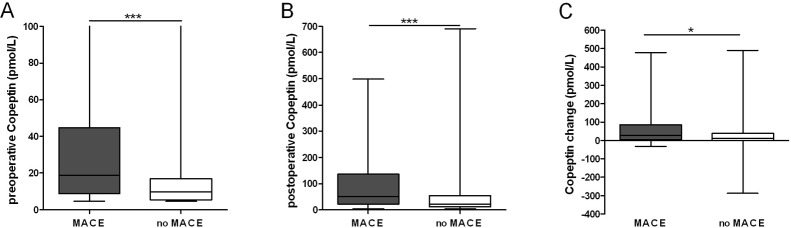
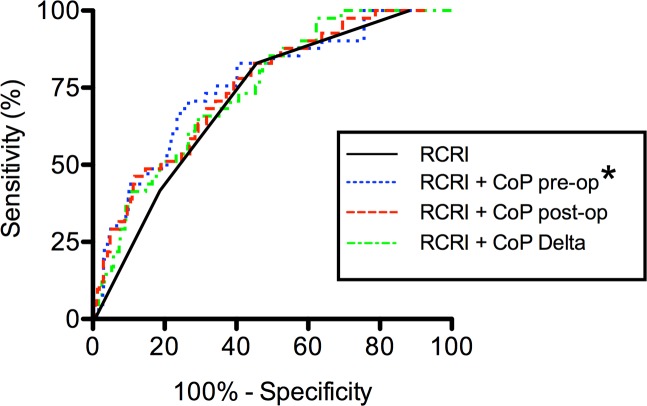
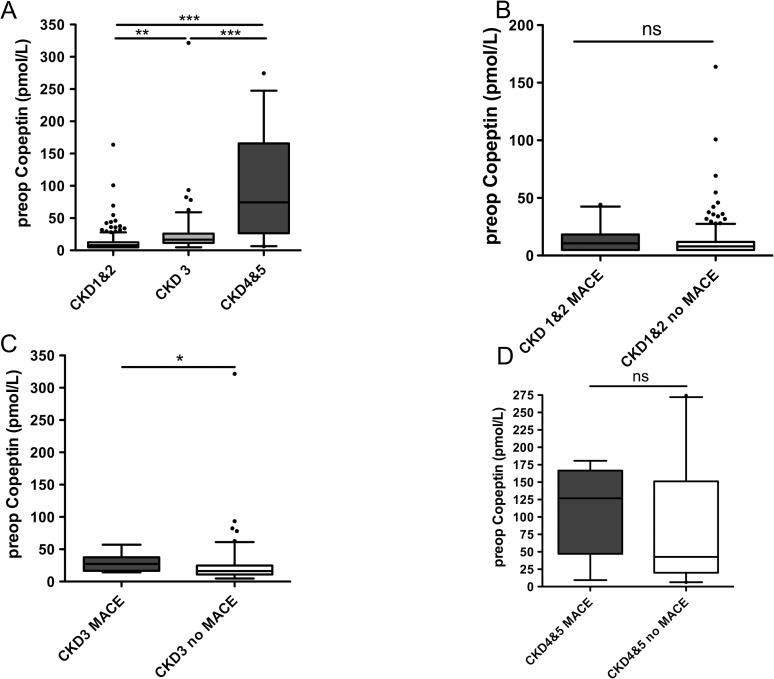
Results: 41 patients reached the primary endpoint, including 63.4% aortic, 26.8% carotid, and 9.8% peripheral surgeries. Linear regression analysis showed that RCRI (P< .001), pre- (P< .001), postoperative Copeptin (P< .001) and Copeptin level change (P= .001) were associated with perioperative MACE, but CKD remained independently associated with MACE and Copeptin levels. Multivariate regression showed that increased Copeptin levels added risk predictive information to the RCRI (P= .003). Especially in the intermediate RCRI categories was Copeptin significantly associated with the occurrence of MACE. (P< .05 Kruskal Wallis test). Subdivision of the study cohort into CKD stages revealed that preoperative Copeptin was significantly associated with CKD stages (P< .0001) and preoperative Copeptin measurements could not predict MACE in patients with more severe CKD stages.
Conclusion: Preoperative Copeptin loses its risk predictive potential for perioperative MACE in patients with chronic kidney disease undergoing vascular surgery.
Conflict of interest statement
Figures
Similar articles
-
The comparative and added prognostic value of biomarkers to the Revised Cardiac Risk Index for preoperative prediction of major adverse cardiac events and all-cause mortality in patients who undergo noncardiac surgery.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD013139. doi: 10.1002/14651858.CD013139.pub2. Cochrane Database Syst Rev. 2021. PMID: 34931303 Free PMC article. Review.
-
The Vascular Study Group of New England Cardiac Risk Index (VSG-CRI) predicts cardiac complications more accurately than the Revised Cardiac Risk Index in vascular surgery patients.J Vasc Surg. 2010 Sep;52(3):674-83, 683.e1-683.e3. doi: 10.1016/j.jvs.2010.03.031. Epub 2010 Jun 8. J Vasc Surg. 2010. PMID: 20570467
-
External validation of the Revised Cardiac Risk Index and update of its renal variable to predict 30-day risk of major cardiac complications after non-cardiac surgery: rationale and plan for analyses of the VISION study.BMJ Open. 2017 Jan 9;7(1):e013510. doi: 10.1136/bmjopen-2016-013510. BMJ Open. 2017. PMID: 28069624 Free PMC article. Clinical Trial.
-
Incremental Value of Preoperative Copeptin for Predicting Myocardial Injury.Anesth Analg. 2016 Dec;123(6):1363-1371. doi: 10.1213/ANE.0000000000001635. Anesth Analg. 2016. PMID: 27870734 Clinical Trial.
-
An update on predictive biomarkers for major adverse cardiovascular events in patients undergoing vascular surgery.J Clin Anesth. 2016 Sep;33:105-16. doi: 10.1016/j.jclinane.2016.03.021. Epub 2016 Apr 29. J Clin Anesth. 2016. PMID: 27555142 Review.
Cited by
-
Elektif Non-Kardiyak Cerrahi Geçirecek Erişkinlerin Pre-Operatif Değerlendirme Kılavuzu: Avrupa Anesteziyoloji Derneği’nden Güncellenmiş Önerilerin Özeti: Pre-Operative Evaluation of Adults Undergoing Elective Noncardiac Surgery: Summary of the Updated Guideline From the European Society of Anaesthesiology.Turk J Anaesthesiol Reanim. 2019 Jun;47(3):244-272. doi: 10.5152/TJAR.2019.150419. Epub 2018 Jun 1. Turk J Anaesthesiol Reanim. 2019. PMID: 31183475 Free PMC article. Turkish. No abstract available.
-
Risk Assessment.Curr Anesthesiol Rep. 2018;8(1):1-8. doi: 10.1007/s40140-018-0246-9. Epub 2018 Jan 30. Curr Anesthesiol Rep. 2018. PMID: 29527132 Free PMC article. Review.
-
Beyond the Limits: Clinical Utility of Novel Cardiac Biomarkers.Biomed Res Int. 2015;2015:187384. doi: 10.1155/2015/187384. Epub 2015 Oct 4. Biomed Res Int. 2015. PMID: 26504786 Free PMC article. Review.
-
The comparative and added prognostic value of biomarkers to the Revised Cardiac Risk Index for preoperative prediction of major adverse cardiac events and all-cause mortality in patients who undergo noncardiac surgery.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD013139. doi: 10.1002/14651858.CD013139.pub2. Cochrane Database Syst Rev. 2021. PMID: 34931303 Free PMC article. Review.
-
Copeptin concentration following cardiac surgery as a prognostic marker of postoperative acute kidney injury: a prospective cohort study.J Thorac Dis. 2020 Nov;12(11):6609-6617. doi: 10.21037/jtd-20-2323. J Thorac Dis. 2020. PMID: 33282362 Free PMC article.
References
-
- Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, et al. (1999) Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 100: 1043–1049. - PubMed
-
- Bertges DJ, Goodney PP, Zhao Y, Schanzer A, Nolan BW, Likosky DS, et al. (2010) The Vascular Study Group of New England Cardiac Risk Index (VSG-CRI) predicts cardiac complications more accurately than the Revised Cardiac Risk Index in vascular surgery patients. Journal of vascular surgery 52: 674–683, 683 e671–683 e673. 10.1016/j.jvs.2010.03.031 - DOI - PubMed
-
- Charpentier S, Maupas-Schwalm F, Cournot M, Elbaz M, Botella JM, Lauque D (2012) Combination of copeptin and troponin assays to rapidly rule out non-ST elevation myocardial infarction in the emergency department. Academic emergency medicine: official journal of the Society for Academic Emergency Medicine 19: 517–524. 10.1111/j.1553-2712.2012.01350.x - DOI - PubMed
-
- Ray P, Charpentier S, Chenevier-Gobeaux C, Reichlin T, Twerenbold R, Claessens YE, et al. (2012) Combined copeptin and troponin to rule out myocardial infarction in patients with chest pain and a history of coronary artery disease. The American journal of emergency medicine 30: 440–448. 10.1016/j.ajem.2011.12.008 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
