

Post-processing of structural MRI for individualized diagnostics
- PMID: 25853079
- PMCID: PMC4379317
- DOI: 10.3978/j.issn.2223-4292.2015.01.10
Post-processing of structural MRI for individualized diagnostics
Abstract
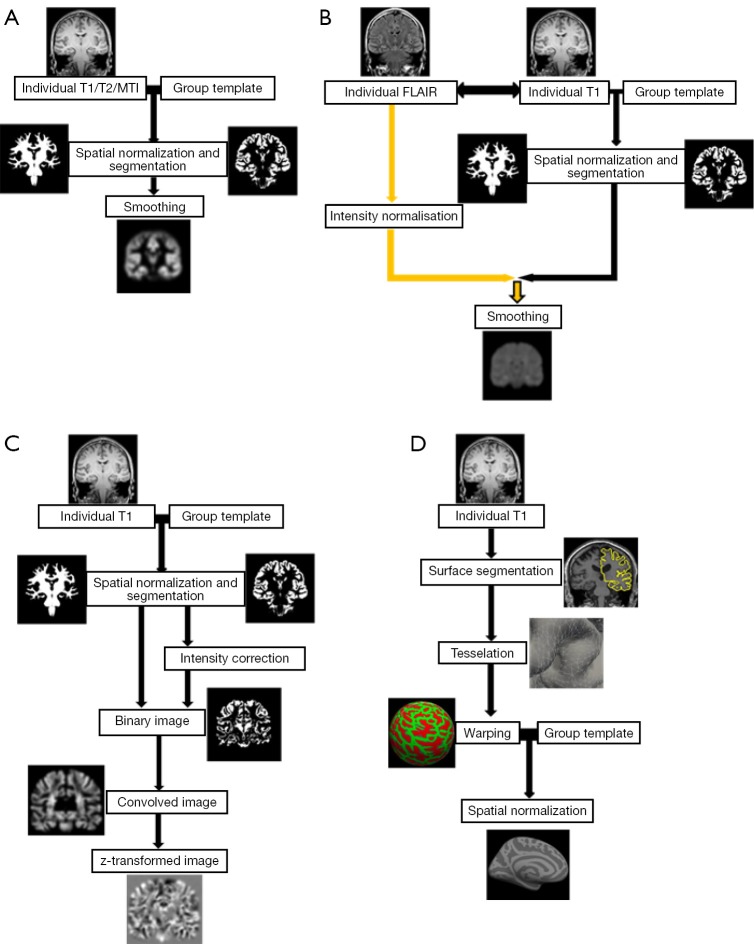
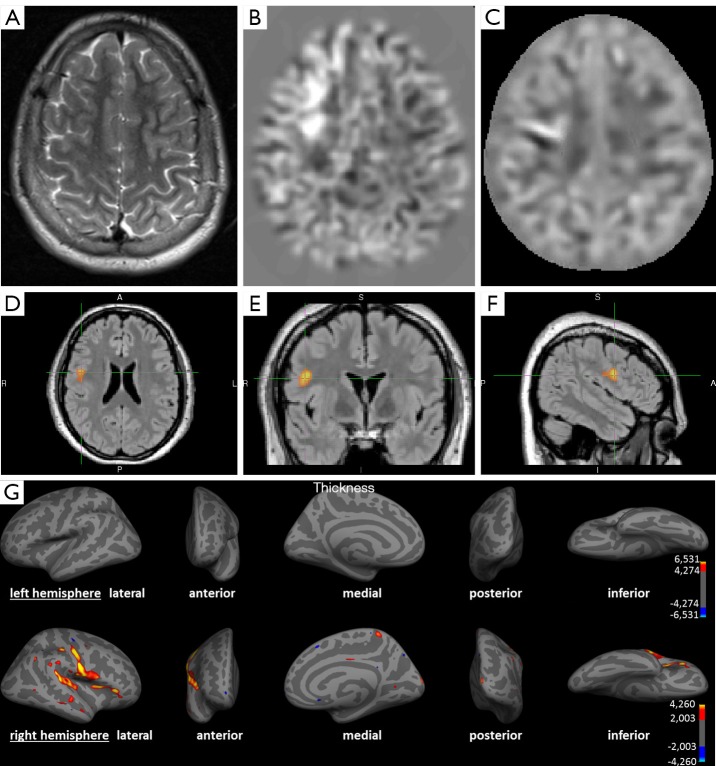
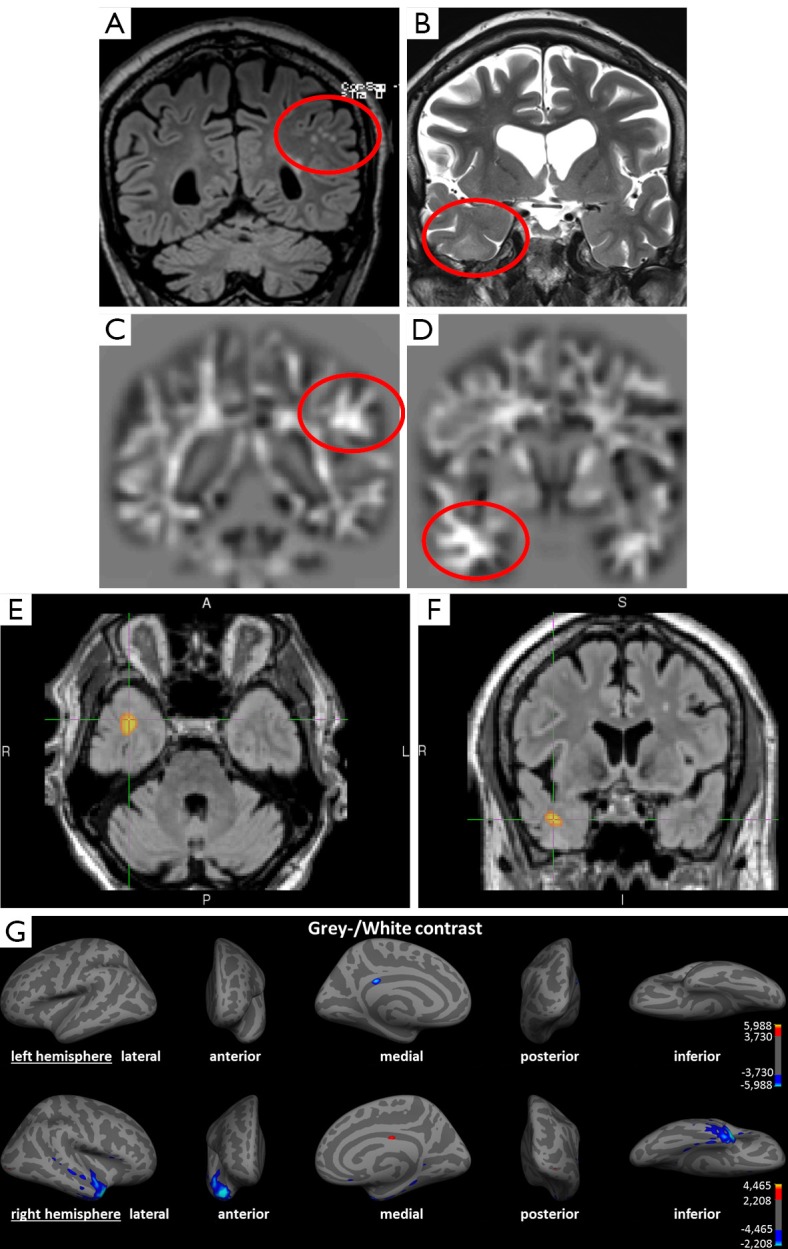
Currently, a relevant proportion of all histopathologically proven focal cortical dysplasia (FCD) escape visual detection; this shows the need for additional improvements in analyzing MRI data. A positive MRI is still the strongest prognostic factor for postoperative freedom of seizures. Among several post-processing methods voxel-based morphometry (VBM) of T1- and T2-weighted sequences and T2 relaxometry are routinely applied in pre-surgical diagnostics of cryptogenic epilepsy in epilepsy centers. VBM is superior to conventional visual analysis with 9-15% more identified epileptogenic foci, while T2 relaxometry has its main application in (mesial) temporal lobe epilepsy. Further methods such as surface-based morphometry (SBM) or diffusion tensor imaging are promising but there is a lack of current studies comparing their individual diagnostic value. Post-processing methods represent an important addition to conventional visual analysis but need to be interpreted with expertise and experience so that they should be apprehended as a complementary tool within the context of the multi-modal evaluation of epilepsy patients. This review will give an overview of existing post-processing methods of structural MRI and outline their clinical relevance in detection of epileptogenic structural changes.
Keywords: Epilepsy; post-processing; voxel-based morphometry (VBM).
Figures
Similar articles
-
The role of voxel-based morphometry in the detection of cortical dysplasia within the temporal pole in patients with intractable mesial temporal lobe epilepsy.Epilepsia. 2012 Jun;53(6):1004-12. doi: 10.1111/j.1528-1167.2012.03456.x. Epub 2012 Apr 17. Epilepsia. 2012. PMID: 22510082
-
Voxel based morphometry of FLAIR MRI in children with intractable focal epilepsy: implications for surgical intervention.Eur J Radiol. 2012 Jun;81(6):1299-305. doi: 10.1016/j.ejrad.2010.12.043. Epub 2011 Jan 15. Eur J Radiol. 2012. PMID: 21242042
-
Computational analysis in epilepsy neuroimaging: A survey of features and methods.Neuroimage Clin. 2016 Feb 23;11:515-529. doi: 10.1016/j.nicl.2016.02.013. eCollection 2016. Neuroimage Clin. 2016. PMID: 27114900 Free PMC article. Review.
-
Comparison of morphometric analysis based on T1- and T2-weighted MRI data for visualization of focal cortical dysplasia.Epilepsy Res. 2013 Oct;106(3):403-9. doi: 10.1016/j.eplepsyres.2013.06.016. Epub 2013 Jul 25. Epilepsy Res. 2013. PMID: 23891304
-
Neuroimaging of focal cortical dysplasia.J Neuroimaging. 2006 Jul;16(3):185-96. doi: 10.1111/j.1552-6569.2006.00025.x. J Neuroimaging. 2006. PMID: 16808819 Review.
Cited by
-
MRI-Based Machine Learning Prediction Framework to Lateralize Hippocampal Sclerosis in Patients With Temporal Lobe Epilepsy.Neurology. 2021 Oct 19;97(16):e1583-e1593. doi: 10.1212/WNL.0000000000012699. Epub 2021 Sep 2. Neurology. 2021. PMID: 34475125 Free PMC article.
-
Novel surface features for automated detection of focal cortical dysplasias in paediatric epilepsy.Neuroimage Clin. 2016 Dec 30;14:18-27. doi: 10.1016/j.nicl.2016.12.030. eCollection 2017. Neuroimage Clin. 2016. PMID: 28123950 Free PMC article.
-
Presurgical epilepsy evaluation and epilepsy surgery.F1000Res. 2019 Oct 29;8:F1000 Faculty Rev-1818. doi: 10.12688/f1000research.17714.1. eCollection 2019. F1000Res. 2019. PMID: 31700611 Free PMC article. Review.
-
Optical tissue clearing associated with 3D imaging: application in preclinical and clinical studies.Histochem Cell Biol. 2022 May;157(5):497-511. doi: 10.1007/s00418-022-02081-5. Epub 2022 Mar 2. Histochem Cell Biol. 2022. PMID: 35235045 Free PMC article. Review.
-
Brain imaging in the assessment for epilepsy surgery.Lancet Neurol. 2016 Apr;15(4):420-33. doi: 10.1016/S1474-4422(15)00383-X. Epub 2016 Feb 24. Lancet Neurol. 2016. PMID: 26925532 Free PMC article. Review.
References
-
- Guerrini R, Sicca F, Parmeggiani L.Epilepsy and malformations of the cerebral cortex. Epileptic Disord 2003;5Suppl 2:S9-26. - PubMed
-
- Cotter D, Honavar M, Lovestone S, Raymond L, Kerwin R, Anderton B, Everall I.Disturbance of Notch-1 and Wnt signalling proteins in neuroglial balloon cells and abnormal large neurons in focal cortical dysplasia in human cortex. Acta Neuropathol 1999;98:465-72. - PubMed
-
- Blümcke I, Thom M, Aronica E, Armstrong DD, Vinters HV, Palmini A, Jacques TS, Avanzini G, Barkovich AJ, Battaglia G, Becker A, Cepeda C, Cendes F, Colombo N, Crino P, Cross JH, Delalande O, Dubeau F, Duncan J, Guerrini R, Kahane P, Mathern G, Najm I, Ozkara C, Raybaud C, Represa A, Roper SN, Salamon N, Schulze-Bonhage A, Tassi L, Vezzani A, Spreafico R. The clinicopathologic spectrum of focal cortical dysplasias: a consensus classification proposed by an ad hoc Task Force of the ILAE Diagnostic Methods Commission. Epilepsia 2011;52:158-74. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources