

Head and neck cancer subtypes with biological and clinical relevance: Meta-analysis of gene-expression data
- PMID: 25821127
- PMCID: PMC4496244
- DOI: 10.18632/oncotarget.3301
Head and neck cancer subtypes with biological and clinical relevance: Meta-analysis of gene-expression data
Abstract
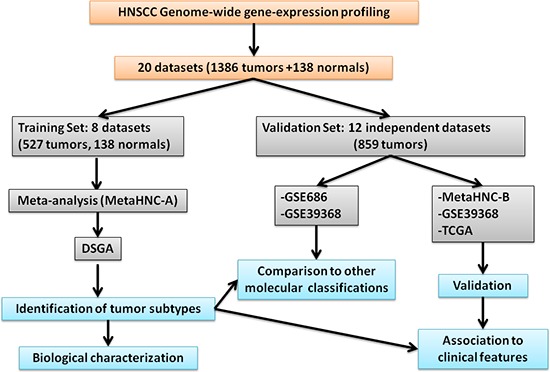
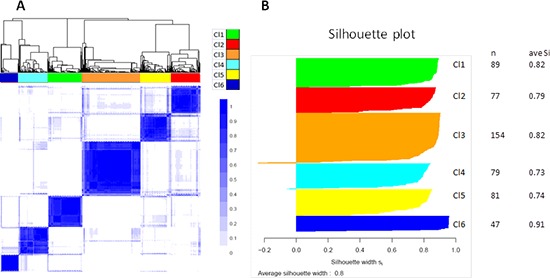
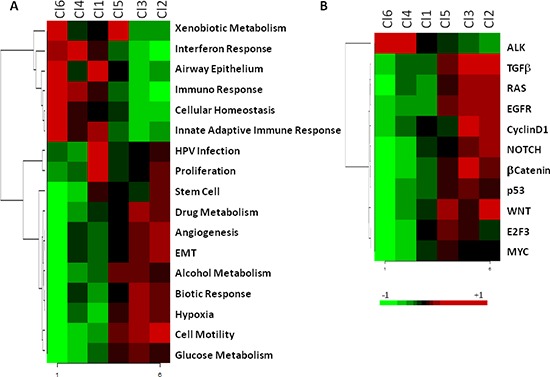
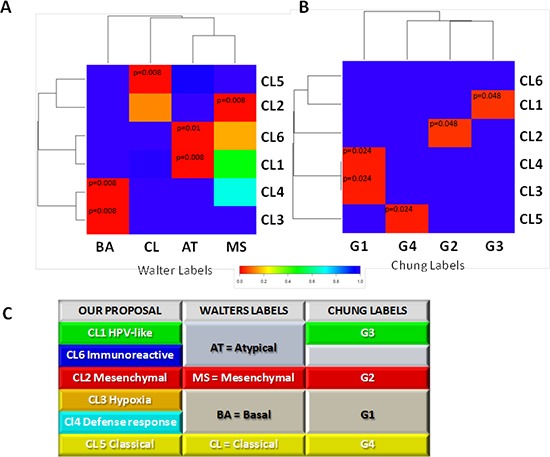
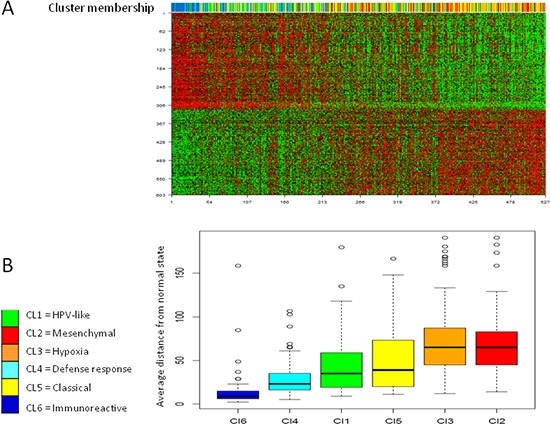
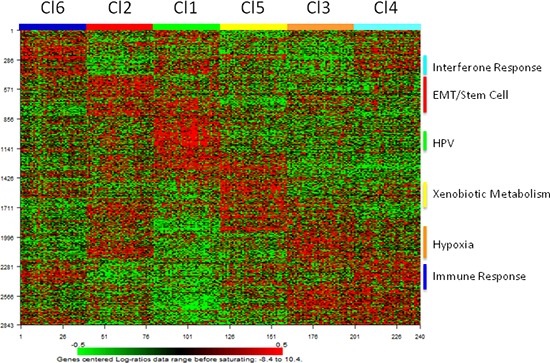
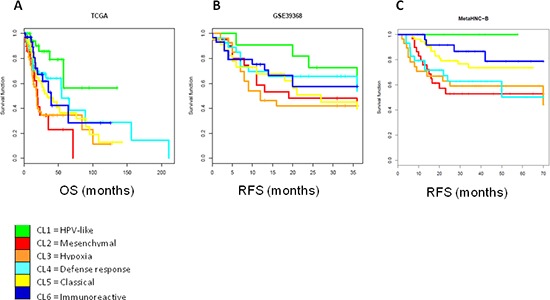
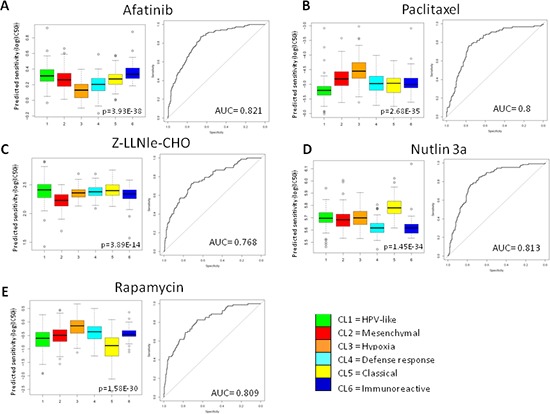
Head and neck squamous cell carcinoma (HNSCC) is a disease with heterogeneous clinical behavior and response to therapies. Despite the introduction of multimodality treatment, 40-50% of patients with advanced disease recur. Therefore, there is an urgent need to improve the classification beyond the current parameters in clinical use to better stratify patients and the therapeutic approaches. Following a meta-analysis approach we built a large training set to whom we applied a Disease-Specific Genomic Analysis (DSGA) to identify the disease component embedded into the tumor data. Eleven independent microarray datasets were used as validation sets. Six different HNSCC subtypes that summarize the aberrant alterations occurring during tumor progression were identified. Based on their main biological characteristics and de-regulated signaling pathways, the subtypes were designed as immunoreactive, inflammatory, human papilloma virus (HPV)-like, classical, hypoxia associated, and mesenchymal. Our findings highlighted a more aggressive behavior for mesenchymal and hypoxia-associated subtypes. The Genomics Drug Sensitivity Project was used to identify potential associations with drug sensitivity and significant differences were observed among the six subtypes. To conclude, we report a robust molecularly defined subtype classification in HNSCC that can improve patient selection and pave the way to the development of appropriate therapeutic strategies.
Keywords: HNSCC; gene expression; meta-analysis; microarray; tumor subtypes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
A 13-gene expression-based radioresistance score highlights the heterogeneity in the response to radiation therapy across HPV-negative HNSCC molecular subtypes.BMC Med. 2017 Sep 1;15(1):165. doi: 10.1186/s12916-017-0929-y. BMC Med. 2017. PMID: 28859688 Free PMC article.
-
Identification of human papillomavirus status specific biomarker in head and neck cancer.Head Neck. 2015 Sep;37(9):1310-8. doi: 10.1002/hed.23751. Epub 2014 Jul 19. Head Neck. 2015. PMID: 24817691
-
Three distinct genomic subtypes of head and neck squamous cell carcinoma associated with clinical outcomes.Oral Oncol. 2018 Oct;85:44-51. doi: 10.1016/j.oraloncology.2018.08.009. Epub 2018 Aug 23. Oral Oncol. 2018. PMID: 30220319
-
The role of Human papillomavirus in head and neck cancer and the impact on radiotherapy outcome.Radiother Oncol. 2010 Jun;95(3):371-80. doi: 10.1016/j.radonc.2010.04.022. Epub 2010 May 20. Radiother Oncol. 2010. PMID: 20493569 Review.
-
Current status of biomarkers in head and neck cancer.J Surg Oncol. 2008 Jun 15;97(8):640-3. doi: 10.1002/jso.21023. J Surg Oncol. 2008. PMID: 18493942 Review.
Cited by
-
Whole-genome CpG-resolution DNA Methylation Profiling of HNSCC Reveals Distinct Mechanisms of Carcinogenesis for Fine-scale HPV+ Cancer Subtypes.Cancer Res Commun. 2023 Aug 30;3(8):1701-1715. doi: 10.1158/2767-9764.CRC-23-0009. eCollection 2023 Aug. Cancer Res Commun. 2023. PMID: 37654626 Free PMC article.
-
Genomics Reloaded: Rise of the Expression Profiles.Int J Radiat Oncol Biol Phys. 2018 May 1;101(1):1-3. doi: 10.1016/j.ijrobp.2017.10.023. Int J Radiat Oncol Biol Phys. 2018. PMID: 29619961 Free PMC article. No abstract available.
-
Meta-Analyses of Microarray Datasets Identifies ANO1 and FADD as Prognostic Markers of Head and Neck Cancer.PLoS One. 2016 Jan 25;11(1):e0147409. doi: 10.1371/journal.pone.0147409. eCollection 2016. PLoS One. 2016. PMID: 26808319 Free PMC article.
-
A comprehensive prognostic score for head and neck squamous cancer driver genes and phenotype traits.Discov Oncol. 2023 Oct 28;14(1):193. doi: 10.1007/s12672-023-00796-y. Discov Oncol. 2023. PMID: 37897503 Free PMC article.
-
Mining of Self-Organizing Map Gene-Expression Portraits Reveals Prognostic Stratification of HPV-Positive Head and Neck Squamous Cell Carcinoma.Cancers (Basel). 2019 Jul 26;11(8):1057. doi: 10.3390/cancers11081057. Cancers (Basel). 2019. PMID: 31357501 Free PMC article.
References
-
- Grégoire V, Lefebvre JL, Licitra L, Felip E, EHNS-ESMO-ESTRO Guidelines Working Group Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21 - PubMed
-
- Carvalho AL, Nishimoto IN, Califano JA, Kowalski LP. Trends in incidence and prognosis for head and neck cancer in the United States: a site-specific analysis of the SEER database. Int J Cancer. 2005;114:806–816. - PubMed
-
- Denaro N, Russi EG, Adamo V, Merlano MC. State-of-the-art and emerging treatment options in the management of head and neck cancer: news from 2013. Oncology. 2014;86:212–229. - PubMed
-
- Sørlie T, Perou CM, Tibshirani R, Aas T, Geisler S, Johnsen H, Hastie T, Eisen MB, van de Rijn M, Jeffrey SS, Thorsen T, Quist H, Matese JC, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA. 2001;98:10869–10874. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
