

Do frequent moderate exacerbations contribute to progression of chronic obstructive pulmonary disease in patients who are ex-smokers?
- PMID: 25792820
- PMCID: PMC4362655
- DOI: 10.2147/COPD.S76475
Do frequent moderate exacerbations contribute to progression of chronic obstructive pulmonary disease in patients who are ex-smokers?
Abstract
Background: In addition to smoking, acute exacerbations are considered to be a contributing factor to progression of chronic obstructive pulmonary disease (COPD). However, these findings come from studies including active smokers, while results in ex-smokers are scarce and contradictory. The purpose of this study was to evaluate if frequent acute moderate exacerbations are associated with an accelerated decline in forced expiratory volume in one second (FEV1) and impairment of functional and clinical outcomes in ex-smoking COPD patients.
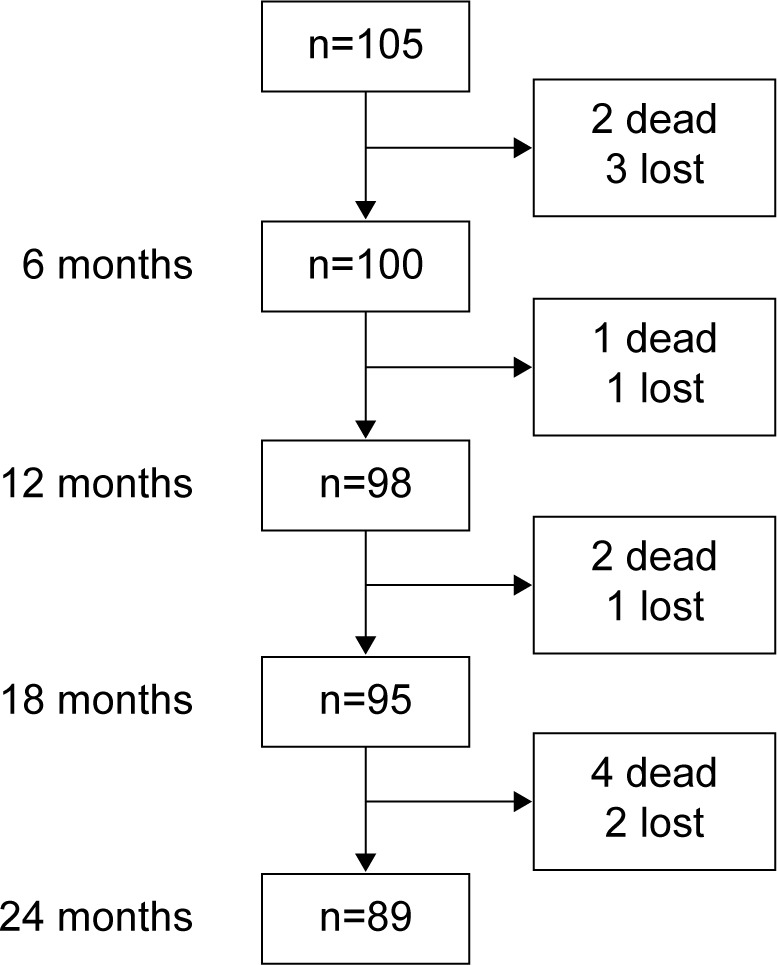
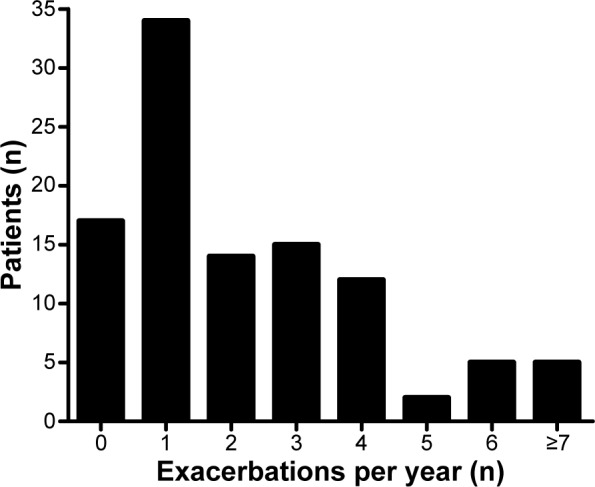
Methods: A cohort of 100 ex-smoking patients recruited for a 2-year follow-up study was evaluated at inclusion and at 6-monthly scheduled visits while in a stable condition. Evaluation included anthropometry, spirometry, inspiratory capacity, peripheral capillary oxygen saturation, severity of dyspnea, a 6-minute walking test, BODE (Body mass index, airflow Obstruction, Dyspnea, Exercise performance) index, and quality of life (St George's Respiratory Questionnaire and Chronic Respiratory Disease Questionnaire). Severity of exacerbation was graded as moderate or severe according to health care utilization. Patients were classified as infrequent exacerbators if they had no or one acute exacerbation/year and frequent exacerbators if they had two or more acute exacerbations/year. Random effects modeling, within hierarchical linear modeling, was used for analysis.
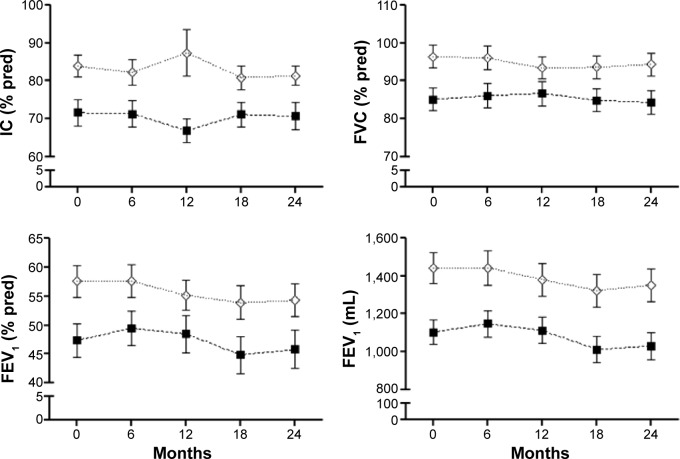
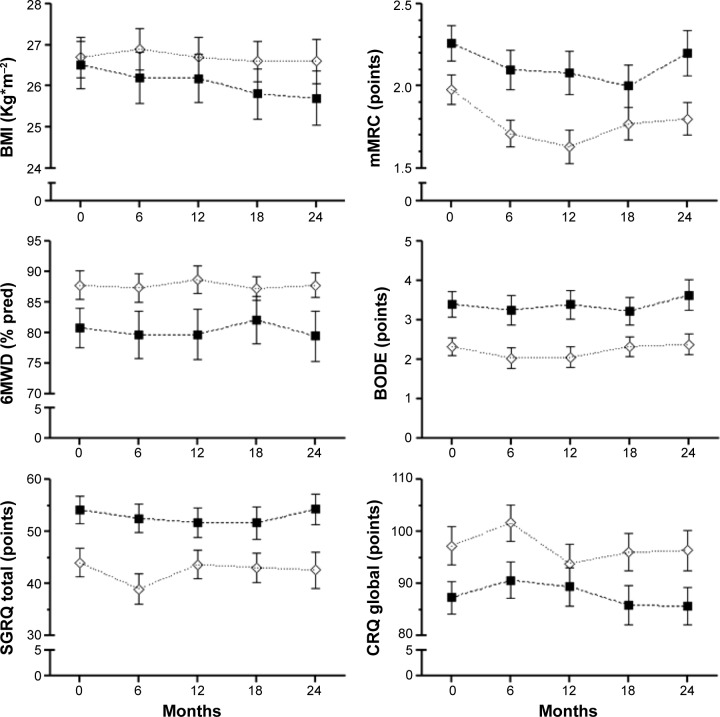
Results: During follow-up, 419 (96% moderate) acute exacerbations were registered. At baseline, frequent exacerbators had more severe disease than infrequent exacerbators according to their FEV1 and BODE index, and also showed greater impairment in inspiratory capacity, forced vital capacity, peripheral capillary oxygen saturation, 6-minute walking test, and quality of life. However, no significant difference in FEV1 decline over time was found between the two groups (54.7±13 mL/year versus 85.4±15.9 mL/year in frequent exacerbators and infrequent exacerbators, respectively). This was also the case for all other measurements.
Conclusion: Our results suggest that frequent moderate exacerbations do not contribute to accelerated clinical and functional decline in COPD patients who are ex-smokers.
Keywords: BODE index; FEV1; acute exacerbations; chronic obstructive pulmonary disease; disease progression; health status.
Figures
Similar articles
-
Exacerbations and lung function decline in COPD: new insights in current and ex-smokers.Respir Med. 2007 Jun;101(6):1305-12. doi: 10.1016/j.rmed.2006.10.012. Epub 2006 Nov 16. Respir Med. 2007. PMID: 17112715
-
Emphysematous phenotype is an independent predictor for frequent exacerbation of COPD.Int J Tuberc Lung Dis. 2014 Dec;18(12):1407-14. doi: 10.5588/ijtld.14.0205. Int J Tuberc Lung Dis. 2014. PMID: 25517804
-
[Systemic inflammation among stable ex smokers with chronic obstructive pulmonary disease].Rev Med Chil. 2010 Aug;138(8):957-64. Epub 2010 Nov 26. Rev Med Chil. 2010. PMID: 21140052 Spanish.
-
The value of forced expiratory volume in 1 second decline in the assessment of chronic obstructive pulmonary disease progression.Am J Med. 2006 Oct;119(10 Suppl 1):4-11. doi: 10.1016/j.amjmed.2006.08.002. Am J Med. 2006. PMID: 16996894 Review.
-
Exacerbations of chronic obstructive pulmonary disease.Respir Care. 2003 Dec;48(12):1204-13; discussion 1213-5. Respir Care. 2003. PMID: 14651761 Review.
Cited by
-
The effects of smoking and smoking cessation on nasal mucociliary clearance, mucus properties and inflammation.Clinics (Sao Paulo). 2016 Jul;71(6):344-50. doi: 10.6061/clinics/2016(06)10. Clinics (Sao Paulo). 2016. PMID: 27438569 Free PMC article.
-
Biomarkers and clinical outcomes in COPD: a systematic review and meta-analysis.Thorax. 2019 May;74(5):439-446. doi: 10.1136/thoraxjnl-2018-211855. Epub 2019 Jan 7. Thorax. 2019. PMID: 30617161 Free PMC article.
-
Improved outcomes in ex-smokers with COPD: a UK primary care observational cohort study.Eur Respir J. 2017 May 23;49(5):1602114. doi: 10.1183/13993003.02114-2016. Print 2017 May. Eur Respir J. 2017. PMID: 28536250 Free PMC article.
References
-
- Anthonisen NR, Connett JE, Murray RP. Smoking and lung function of Lung Health Study participants after 11 years. Am J Respir Crit Care Med. 2002;166(5):675–679. - PubMed
-
- Cote CG, Doderlly LJ, Celli BR. Impact of COPD exacerbations on patient-centered outcomes. Chest. 2007;131(3):696–704. - PubMed
-
- Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbations on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1418–1422. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
