

Stroke warning campaigns: delivering better patient outcomes? A systematic review
- PMID: 25750550
- PMCID: PMC4348144
- DOI: 10.2147/PROM.S54087
Stroke warning campaigns: delivering better patient outcomes? A systematic review
Abstract
Background: Patient delay in presenting to hospital with stroke symptoms remains one of the major barriers to thrombolysis treatment, leading to its suboptimal use internationally. Educational interventions such as mass media campaigns and community initiatives aim to reduce patient delays by promoting the signs and symptoms of a stroke, but no consistent evidence exists to show that such interventions result in appropriate behavioral responses to stroke symptoms.
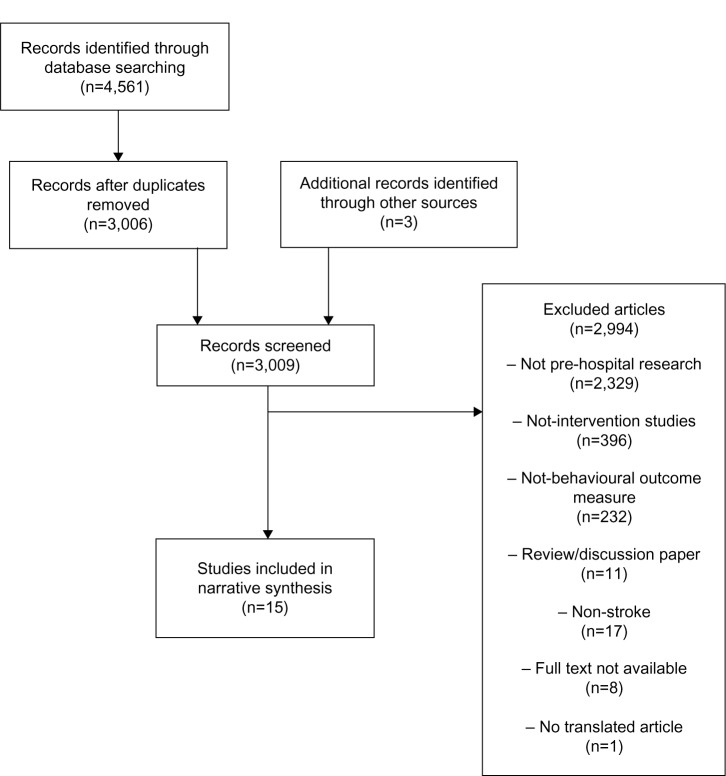
Methods: A systematic literature search and narrative synthesis were conducted to examine whether public educational interventions were successful in the reduction of patient delay to hospital presentation with stroke symptoms. Three databases, MEDLINE, CINAHL, and PsycINFO, were searched to identify quantitative studies with measurable behavioral end points, including time to hospital presentation, thrombolysis rates, ambulance use, and emergency department (ED) presentations with stroke.
Results: Fifteen studies met the inclusion criteria: one randomized controlled trial, two time series analyses, three controlled before and after studies, five uncontrolled before and after studies, two retrospective observational studies, and two prospective observational studies. Studies were heterogeneous in quality; thus, meta-analysis was not feasible. Thirteen studies examined prehospital delay, with ten studies reporting a significant reduction in delay times, with a varied magnitude of effect. Eight studies examined thrombolysis rates, with only three studies reporting a statistically significant increase in thrombolysis administration. Five studies examined ambulance usage, and four reported a statistically significant increase in ambulance transports following the intervention. Three studies examining ED presentations reported significantly increased ED presentations following intervention. Public educational interventions varied widely on type, duration, and content, with description of intervention development largely absent from studies, limiting the potential replication of successful interventions.
Conclusions: Positive intervention effects were reported in the majority of studies; however, methodological weaknesses evident in a number of studies limited the generalizability of the observed effects. Reporting of specific intervention design was suboptimal and impeded the identification of key intervention components for reducing patient delay. The parallel delivery of public and professional interventions further limited the identification of successful intervention components. A lack of studies of sound methodological quality using, at a minimum, a controlled before and after design was identified in this review, and thus studies incorporating a rigorous study design are required to strengthen the evidence for public interventions to reduce patient delay in stroke. The potential clinical benefits of public interventions are far-reaching, and the challenge remains in translating knowledge improvements and correct behavioral intentions to appropriate behavior when stroke occurs.
Keywords: acute stroke treatment; interventions; onset to door times; prehospital delay; professional education; public education.
Figures
Similar articles
-
Behavioral and Pharmacotherapy Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults: An Updated Systematic Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. PMID: 30354042 Free Books & Documents. Review.
-
Behavioral Counseling to Promote a Healthful Diet and Physical Activity for Cardiovascular Disease Prevention in Adults Without Known Cardiovascular Disease Risk Factors: Updated Systematic Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2017 Jul. Report No.: 15-05222-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2017 Jul. Report No.: 15-05222-EF-1. PMID: 29364620 Free Books & Documents. Review.
-
Primary Care Interventions to Prevent Motor Vehicle Occupant Injuries [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2007 Aug. Report No.: 07-05103-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2007 Aug. Report No.: 07-05103-EF-1. PMID: 20722149 Free Books & Documents. Review.
-
The effectiveness of internet-based e-learning on clinician behavior and patient outcomes: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):52-64. doi: 10.11124/jbisrir-2015-1919. JBI Database System Rev Implement Rep. 2015. PMID: 26447007
-
The association between ethnicity and delay in seeking medical care for chest pain: a systematic review.JBI Database System Rev Implement Rep. 2016 Jul;14(7):208-35. doi: 10.11124/JBISRIR-2016-003012. JBI Database System Rev Implement Rep. 2016. PMID: 27532797 Review.
Cited by
-
Knowledge on Signs and Risk Factors in Stroke Patients.J Clin Med. 2020 Aug 7;9(8):2557. doi: 10.3390/jcm9082557. J Clin Med. 2020. PMID: 32784554 Free PMC article.
-
Stroke 112: A Universal Stroke Awareness Program to Reduce Language and Response Barriers.Stroke. 2018 Jul;49(7):1766-1769. doi: 10.1161/STROKEAHA.118.021729. Epub 2018 Jun 20. Stroke. 2018. PMID: 29925649 Free PMC article.
-
Hip Hop Stroke: Study Protocol for a Randomized Controlled Trial to Address Stroke Literacy.J Clin Trials. 2015 Oct;5(5):242. doi: 10.4172/2167-0870.1000242. Epub 2015 Oct 23. J Clin Trials. 2015. PMID: 26779395 Free PMC article.
-
Community Interventions to Increase Stroke Preparedness and Acute Stroke Treatment Rates.Curr Atheroscler Rep. 2017 Nov 16;19(12):64. doi: 10.1007/s11883-017-0695-5. Curr Atheroscler Rep. 2017. PMID: 29147858 Review.
-
Acute stroke alert activation, emergency service use, and reperfusion therapy in Sweden.Brain Behav. 2017 Mar 15;7(4):e00654. doi: 10.1002/brb3.654. eCollection 2017 Apr. Brain Behav. 2017. PMID: 28413705 Free PMC article.
References
-
- Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischaemic stroke. NEMJ. 2008;359:1317–1329. - PubMed
-
- Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375:1695–1703. - PubMed
-
- Schumacher HC, Bateman BT, Boden-Albala B, et al. Use of thrombolysis in acute ischaemic stroke: analysis of the Nationwide Inpatient Sample 1999–2004. Ann Emerg Med. 2007;50:99–107. - PubMed
-
- Evenson KR, Rosamond WD, Morris DL. Prehospital and in-hospital delays in acute stroke care. Neuroepidemiology. 2001;20:65–76. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
