

Contribution of Beta-HPV Infection and UV Damage to Rapid-Onset Cutaneous Squamous Cell Carcinoma during BRAF-Inhibition Therapy
- PMID: 25724524
- PMCID: PMC4452444
- DOI: 10.1158/1078-0432.CCR-14-2667
Contribution of Beta-HPV Infection and UV Damage to Rapid-Onset Cutaneous Squamous Cell Carcinoma during BRAF-Inhibition Therapy
Abstract
Purpose: BRAF-inhibition (BRAFi) therapy for advanced melanoma carries a high rate of secondary cutaneous squamous cell carcinoma (cSCC) and risk of other cancers. UV radiation and α-genus human papillomavirus (HPV) are highly associated with SCC, but a novel role for β-genus HPV is suspected in BRAFi-cSCC. Cutaneous β-HPV may act in concert with host and environmental factors in BRAFi-cSCC.
Experimental design: Primary BRAFi-cSCC tissue DNA isolated from patients receiving vemurafenib or dabrafenib from two cancer centers was analyzed for the presence of cutaneous oncogenic viruses and host genetic mutations. Diagnostic specimens underwent consensus dermatopathology review. Clinical parameters for UV exposure and disease course were statistically analyzed in conjunction with histopathology.
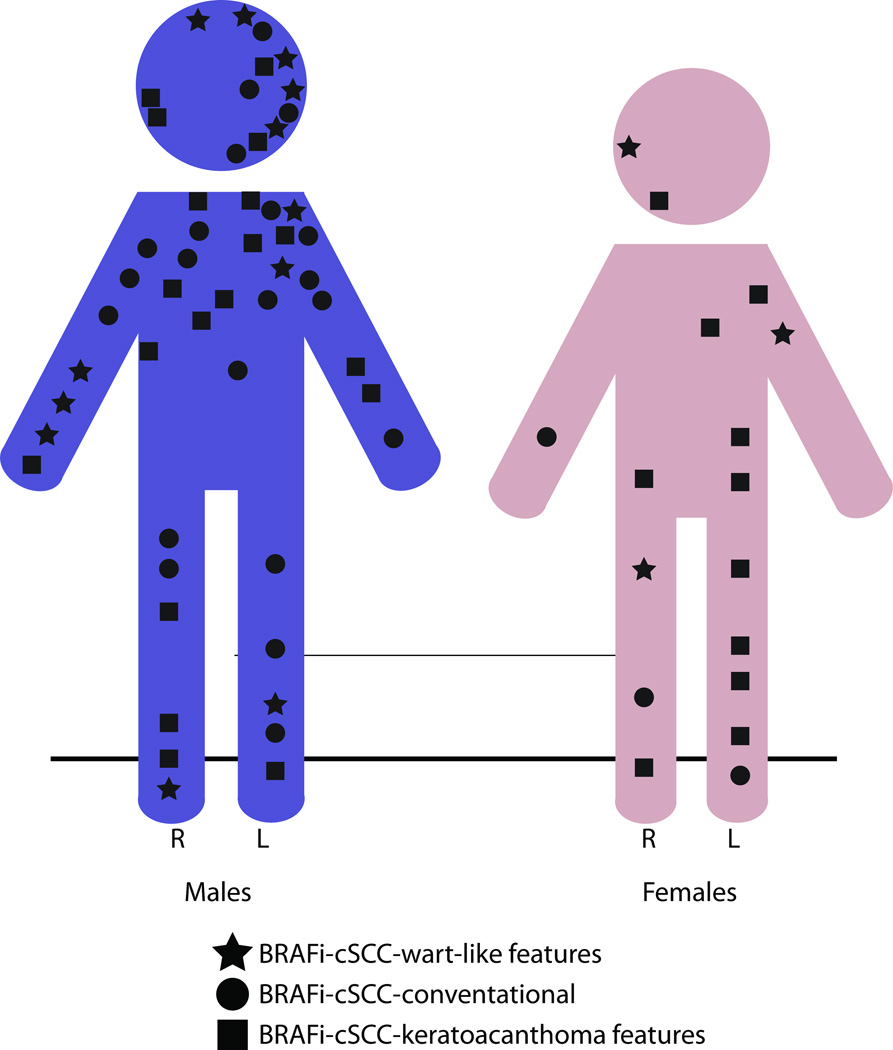
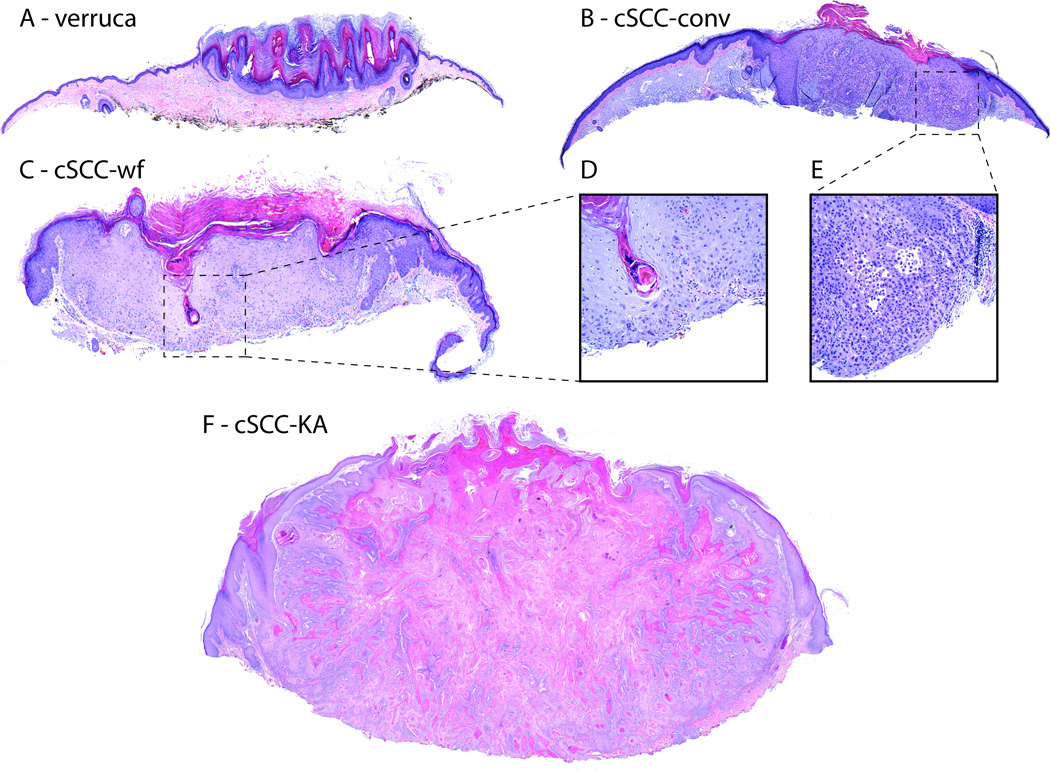
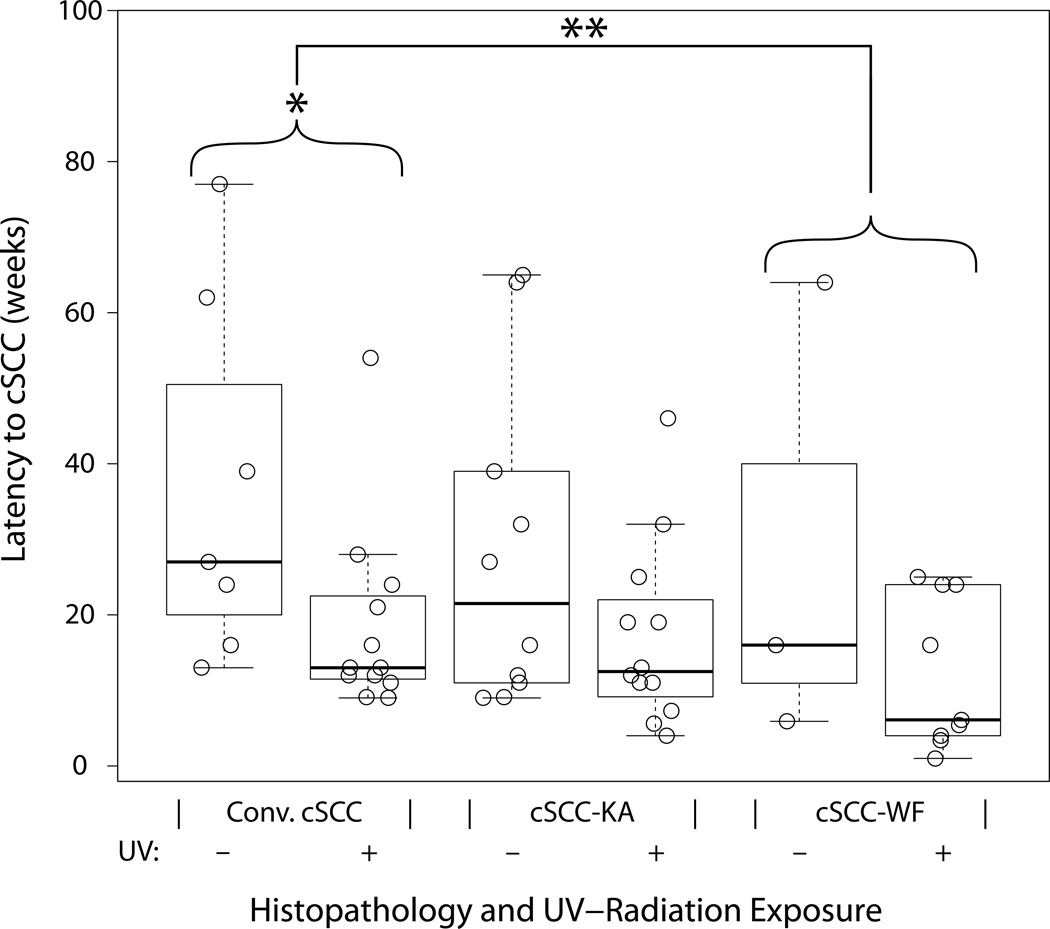
Results: Twenty-nine patients contributed 69 BRAFi-cSCC lesions. BRAFi-cSCC had wart-like features (BRAFi-cSCC-WF) in 22% of specimens. During vemurafenib therapy, BRAFi-cSCC-WF arose 11.6 weeks more rapidly than conventional cSCC when controlled for gender and UV exposure (P value = 0.03). Among all BRAFi-cSCC, β-genus HPV-17, HPV-38, HPV-111 were most frequently isolated, and novel β-HPV genotypes were discovered (CTR, CRT-11, CRT-22). Sequencing revealed 63% of evaluated BRAFi-cSCCs harbored RAS mutations with PIK3CA, CKIT, ALK, and EGFR mutations also detected.
Conclusions: We examined clinical, histopathologic, viral, and genetic parameters in BRAFi-cSCC demonstrating rapid onset; wart-like histomorphology; β-HPV-17, HPV-38, and HPV-111 infection; UV damage; and novel ALK and CKIT mutations. Discovered β-HPV genotypes expand the spectrum of tumor-associated viruses. These findings enhance our understanding of factors cooperating with BRAF inhibition that accelerate keratinocyte oncogenesis as well as broaden the knowledge base of multifactorial mediators of cancer in general.
©2015 American Association for Cancer Research.
Figures
Similar articles
-
Inactivation of TGFβ receptors in stem cells drives cutaneous squamous cell carcinoma.Nat Commun. 2016 Aug 25;7:12493. doi: 10.1038/ncomms12493. Nat Commun. 2016. PMID: 27558455 Free PMC article.
-
COX-2 inhibition prevents the appearance of cutaneous squamous cell carcinomas accelerated by BRAF inhibitors.Mol Oncol. 2014 Mar;8(2):250-60. doi: 10.1016/j.molonc.2013.11.005. Epub 2013 Dec 1. Mol Oncol. 2014. PMID: 24345644 Free PMC article.
-
RAS mutations are associated with the development of cutaneous squamous cell tumors in patients treated with RAF inhibitors.J Clin Oncol. 2012 Jan 20;30(3):316-21. doi: 10.1200/JCO.2011.36.7680. Epub 2011 Nov 7. J Clin Oncol. 2012. PMID: 22067401 Free PMC article.
-
An Emerging Issue in Oncogenic Virology: the Role of Beta Human Papillomavirus Types in the Development of Cutaneous Squamous Cell Carcinoma.J Virol. 2019 Mar 21;93(7):e01003-18. doi: 10.1128/JVI.01003-18. Print 2019 Apr 1. J Virol. 2019. PMID: 30700603 Free PMC article. Review.
-
Molecular mechanisms of human papilloma virus related skin cancers: A review.Medicine (Baltimore). 2024 May 24;103(21):e38202. doi: 10.1097/MD.0000000000038202. Medicine (Baltimore). 2024. PMID: 38787972 Free PMC article. Review.
Cited by
-
Cutaneous Squamous Cell Carcinoma: From Biology to Therapy.Int J Mol Sci. 2020 Apr 22;21(8):2956. doi: 10.3390/ijms21082956. Int J Mol Sci. 2020. PMID: 32331425 Free PMC article. Review.
-
The Role of Senescent Cells in Acquired Drug Resistance and Secondary Cancer in BRAFi-Treated Melanoma.Cancers (Basel). 2021 May 7;13(9):2241. doi: 10.3390/cancers13092241. Cancers (Basel). 2021. PMID: 34066966 Free PMC article. Review.
-
Human polyomaviruses and cancer: an overview.Clinics (Sao Paulo). 2018 Oct 11;73(suppl 1):e558s. doi: 10.6061/clinics/2018/e558s. Clinics (Sao Paulo). 2018. PMID: 30328951 Free PMC article. Review.
-
Betapapillomaviruses in p16-Negative Vulvar Intraepithelial Lesions Associated with Squamous Cell Carcinoma.Viruses. 2023 Sep 19;15(9):1950. doi: 10.3390/v15091950. Viruses. 2023. PMID: 37766356 Free PMC article.
-
The contribution of human papilloma virus infection to cutaneous squamous cell carcinoma in patients with chronic lymphocytic leukemia.EJHaem. 2021 Mar 4;2(2):228-235. doi: 10.1002/jha2.181. eCollection 2021 May. EJHaem. 2021. PMID: 35845291 Free PMC article.
References
-
- Long GV, Trefzer U, Davies MA, Kefford RF, Ascierto PA, Chapman PB, et al. Dabrafenib in patients with Val600Glu or Val600Lys BRAF-mutant melanoma metastatic to the brain (BREAK-MB): A multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13(11):1087–1095. - PubMed
-
- Cohen DN, Chappell JD, Robbins JB. Squamous cell carcinoma in BRAF-inhibitor-treated melanoma patients.In abstracts presented at the 15th Joint Meeting of the International Society of Dermatopathology, March 14–15, San Diego, CA, USA. Amer J Dermatopath. 2012;34(5):e55–e72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
