

Distribution and determinants of cytomegalovirus induced end organ disease/s among people living with HIV/AIDS in a poor resource setting: observation from India
- PMID: 25679798
- PMCID: PMC4332476
- DOI: 10.1371/journal.pone.0117466
Distribution and determinants of cytomegalovirus induced end organ disease/s among people living with HIV/AIDS in a poor resource setting: observation from India
Abstract
Background: In India, despite well-established anti-retroviral treatment programs, Cytomegalovirus (CMV) infection-related end-organ diseases (EODs) still remain a major concern resulting in exacerbation of morbidity and mortality among HIV/AIDS patients. A prospective study was designed to understand the distribution and prognosis of CMV associated EODs and to determine a standardized cut-off value for serum CMV viral load associated with the development of EODs amongst HIV/AIDS subjects.
Methods: In a cohort of 400 late-diagnosed HAART naïve HIV/AIDS subjects attending anti-retroviral centers of Kolkata during 2008-2014, the median duration of follow-up was 560 days, and at least 3 visits subsequent to the baseline were mandatory for eligibility. HIV-1 and CMV viral load were estimated by performing Real-Time Polymerase Chain Reactions (PCR).
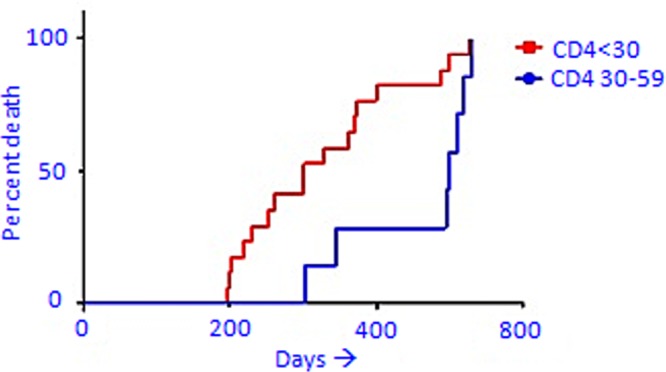
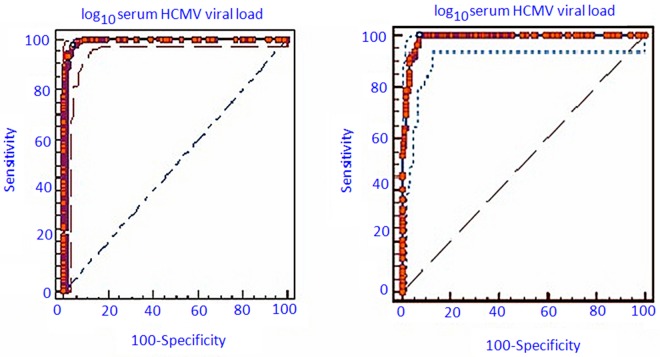
Results: Among subjects, 40.5% (162/400) had CMV EODs which were more common at lower CD4 counts. Poor prognosis and higher death rate were associated with a low CD4 count and increased HIV-1 and CMV viral loads. Subjects having higher CD4 count responded better to therapy [for CD4 = 60-100: Risk Ratio:RR = 1.48 (95% Confidence Interval: 95%CI = 1.18-1.82) and for CD4 = 30-59: RR = 1.64 (95%CI = 1.18-2.27)]. The cut off value of the serum CMV viral load (expressed as log10DNA/ml serum) associated with the development of EODs and disseminated CMV EODs was determined as 5.4 (p<0.0001) and 6.4 (p<0.0001) respectively. These cut offs were found to have satisfactorily high sensitivity, specificity, positive and negative predictive values.
Conclusion: Prognosis of CMV EOD was poor as indicated by higher death rates among subjects with lower CD4 count, and specific cut-off values were found to have useful potential for identification and treatment of CMV infected HIV/AIDS patients in due time to avoid CMV EODs among HIV/AIDS subjects. Targeted intervention programs seemed to be required urgently to make these cut-offs operational in order to minimize the burden of CMV EOD in this vulnerable population.
Conflict of interest statement
Figures

Similar articles
-
Cytomegalovirus viremia, mortality, and end-organ disease among patients with AIDS receiving potent antiretroviral therapies.J Acquir Immune Defic Syndr. 2005 Apr 15;38(5):538-44. doi: 10.1097/01.qai.0000155204.96973.c3. J Acquir Immune Defic Syndr. 2005. PMID: 15793363
-
Plasma cytomegalovirus DNA, pp65 antigenaemia and a low CD4 cell count remain risk factors for cytomegalovirus disease in patients receiving highly active antiretroviral therapy.AIDS. 2000 May 26;14(8):1041-9. doi: 10.1097/00002030-200005260-00017. AIDS. 2000. PMID: 10853987 Clinical Trial.
-
Low rate of CMV end-organ disease in HIV-infected patients despite low CD4+ cell counts and CMV viremia: results of ACTG protocol A5030.HIV Clin Trials. 2009 May-Jun;10(3):143-52. doi: 10.1310/hct1003-143. HIV Clin Trials. 2009. PMID: 19632953 Free PMC article. Clinical Trial.
-
Review of cytomegalovirus coinfection in HIV-infected individuals in Africa.Rev Med Virol. 2017 Jan;27(1). doi: 10.1002/rmv.1907. Epub 2016 Oct 7. Rev Med Virol. 2017. PMID: 27714898 Review.
-
Viruses causing diarrhoea in AIDS.Novartis Found Symp. 2001;238:276-83; discussion 283-8. doi: 10.1002/0470846534.ch17. Novartis Found Symp. 2001. PMID: 11444032 Review.
Cited by
-
Mismatched related vs matched unrelated donors in TCRαβ/CD19-depleted HSCT for primary immunodeficiencies.Blood. 2019 Nov 14;134(20):1755-1763. doi: 10.1182/blood.2019001757. Blood. 2019. PMID: 31558465 Free PMC article. Clinical Trial.
-
Multisystem cytomegalovirus end-organ disease in a patient with advanced HIV.S Afr J Infect Dis. 2022 Nov 11;37(1):468. doi: 10.4102/sajid.v37i1.468. eCollection 2022. S Afr J Infect Dis. 2022. PMID: 36483572 Free PMC article.
-
Routine Immediate Eye Examination at the Point of Care for Diagnosis of AIDS-Related Cytomegalovirus Retinitis Among Patients With a CD4 Count <100 in Myanmar.Open Forum Infect Dis. 2019 Jun 14;6(7):ofz280. doi: 10.1093/ofid/ofz280. eCollection 2019 Jul. Open Forum Infect Dis. 2019. PMID: 31304189 Free PMC article.
References
-
- Brooks GF, Butel JS, Morse SA (2007) Jawetz, Melnick, & Adelberg’s Med Microbiol.: McGraw-Hill Medical; New York, NY, USA: 428–451 p.
-
- d’Arminio Monforte A, Mainini F, Testa L, Vago L, Balotta L, et al. (1997) Predictors of cytomegalovirus disease, natural history and autopsy findings in a cohort of patients with AIDS. AIDS 11: 517–524. - PubMed
-
- Drew WL (1992) Cytomegalovirus infection in patients with AIDS. Clin Infect Dis: 608–615. - PubMed
-
- Goodgame RW (1993) Gastrointestinal cytomegalovirus disease. Ann Int Med 119: 924–935. - PubMed
-
- Jabs DA, Enger C, Bartlett JG (1989) Cytomegalovirus retinitis and acquired immunodeficiency syndrome. Arch Ophth 107: 75–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
