

Middle East respiratory syndrome: An emerging coronavirus infection tracked by the crowd
- PMID: 25656066
- PMCID: PMC7114422
- DOI: 10.1016/j.virusres.2015.01.021
Middle East respiratory syndrome: An emerging coronavirus infection tracked by the crowd
Abstract
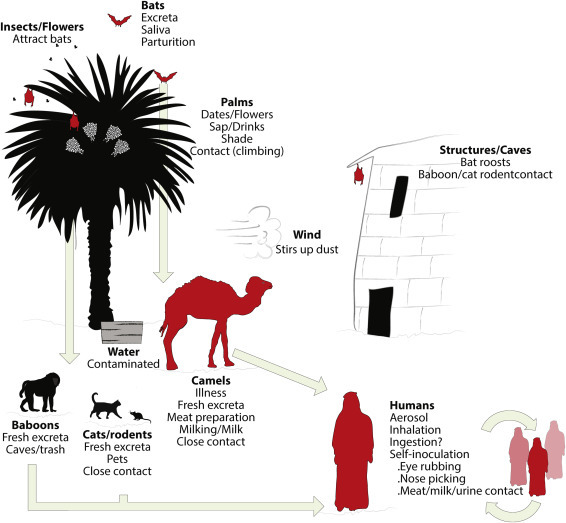
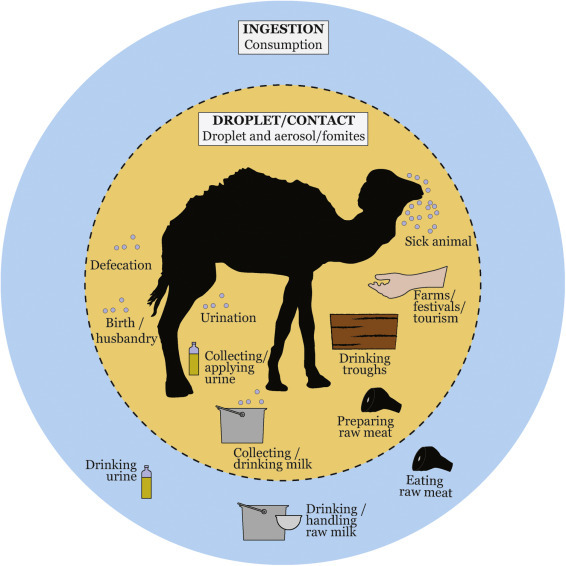
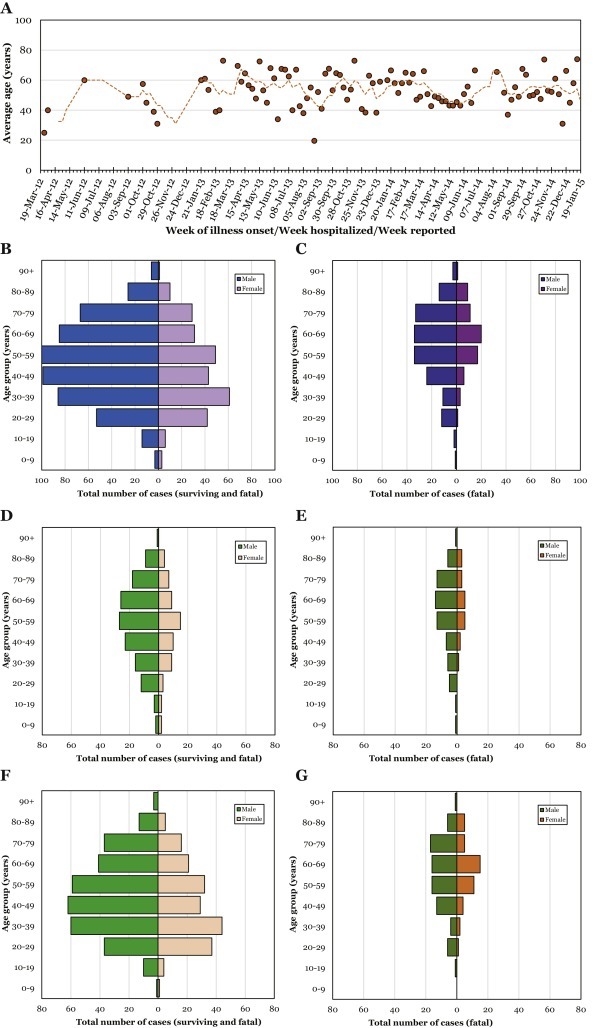
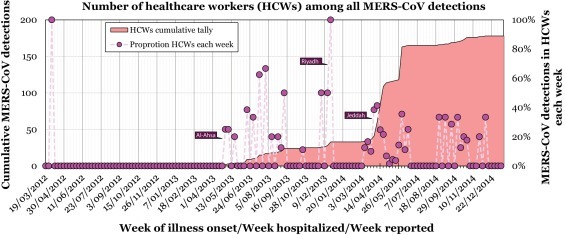
In 2012 in Jordan, infection by a novel coronavirus (CoV) caused the first known cases of Middle East respiratory syndrome (MERS). MERS-CoV sequences have since been found in a bat and the virus appears to be enzootic among dromedary camels across the Arabian Peninsula and in parts of Africa. The majority of human cases have occurred in the Kingdom of Saudi Arabia (KSA). In humans, the etiologic agent, MERS-CoV, has been detected in severe, mild and influenza-like illness and in those without any obvious signs or symptoms of disease. MERS is often a lower respiratory tract disease associated with fever, cough, breathing difficulties, pneumonia that can progress to acute respiratory distress syndrome, multiorgan failure and death among more than a third of those infected. Severe disease is usually found in older males and comorbidities are frequently present in cases of MERS. Compared to SARS, MERS progresses more rapidly to respiratory failure and acute kidney injury, is more often observed as severe disease in patients with underlying illnesses and is more often fatal. MERS-CoV has a broader tropism than SARS-CoV, rapidly triggers cellular damage, employs a different receptor and induces a delayed proinflammatory response in cells. Most human cases have been linked to lapses in infection prevention and control in healthcare settings, with a fifth of virus detections reported among healthcare workers. This review sets out what is currently known about MERS and the MERS-CoV, summarises the new phenomenon of crowd-sourced epidemiology and lists some of the many questions that remain unanswered, nearly three years after the first reported case.
Keywords: Camel; Emerging infectious disease; Healthcare worker; MERS; MERS-CoV; Zoonosis.
Copyright © 2015 Elsevier B.V. All rights reserved.
Figures


Similar articles
-
Middle East respiratory syndrome coronavirus (MERS-CoV): animal to human interaction.Pathog Glob Health. 2015;109(8):354-62. doi: 10.1080/20477724.2015.1122852. Pathog Glob Health. 2015. PMID: 26924345 Free PMC article. Review.
-
MERS coronavirus: diagnostics, epidemiology and transmission.Virol J. 2015 Dec 22;12:222. doi: 10.1186/s12985-015-0439-5. Virol J. 2015. PMID: 26695637 Free PMC article. Review.
-
Evidence for zoonotic origins of Middle East respiratory syndrome coronavirus.J Gen Virol. 2016 Feb;97(2):274-280. doi: 10.1099/jgv.0.000342. Epub 2015 Nov 13. J Gen Virol. 2016. PMID: 26572912 Free PMC article. Review.
-
Limited Genetic Diversity Detected in Middle East Respiratory Syndrome-Related Coronavirus Variants Circulating in Dromedary Camels in Jordan.Viruses. 2021 Mar 31;13(4):592. doi: 10.3390/v13040592. Viruses. 2021. PMID: 33807288 Free PMC article.
-
Enzootic patterns of Middle East respiratory syndrome coronavirus in imported African and local Arabian dromedary camels: a prospective genomic study.Lancet Planet Health. 2019 Dec;3(12):e521-e528. doi: 10.1016/S2542-5196(19)30243-8. Epub 2019 Dec 16. Lancet Planet Health. 2019. PMID: 31843456 Free PMC article.
Cited by
-
Subversion of autophagy machinery and organelle-specific autophagy by SARS-CoV-2 and coronaviruses.Autophagy. 2023 Apr;19(4):1055-1069. doi: 10.1080/15548627.2022.2116677. Epub 2022 Aug 31. Autophagy. 2023. PMID: 36005882 Free PMC article. Review.
-
A Review of Zoonotic Pathogens of Dromedary Camels.Ecohealth. 2019 Jun;16(2):356-377. doi: 10.1007/s10393-019-01413-7. Epub 2019 May 28. Ecohealth. 2019. PMID: 31140075 Free PMC article. Review.
-
Complete Genome Sequence of Middle East Respiratory Syndrome Coronavirus KOR/KNIH/002_05_2015, Isolated in South Korea.Genome Announc. 2015 Aug 13;3(4):e00787-15. doi: 10.1128/genomeA.00787-15. Genome Announc. 2015. PMID: 26272558 Free PMC article.
-
Middle East respiratory syndrome coronavirus (MERS-CoV): animal to human interaction.Pathog Glob Health. 2015;109(8):354-62. doi: 10.1080/20477724.2015.1122852. Pathog Glob Health. 2015. PMID: 26924345 Free PMC article. Review.
-
Middle East respiratory coronavirus (MERS-CoV) spike (S) protein vesicular stomatitis virus pseudoparticle neutralization assays offer a reliable alternative to the conventional neutralization assay in human seroepidemiological studies.Access Microbiol. 2019 Sep 11;1(9):e000057. doi: 10.1099/acmi.0.000057. eCollection 2019. Access Microbiol. 2019. PMID: 32974558 Free PMC article.
References
-
- 2014. Alferon® N Effective Against MERS (Middle East Respiratory Syndrome) Virus In-Vitro. http://www.hemispherx.net/content/investor/default.asp?goto=781.
-
- Aburizaiza A.S., Mattes F.M., Azhar E.I., Hassan A.M., Memish Z.A., Muth D., Meyer B., Lattwein E., Muller M.A., Drosten C. Investigation of anti-middle East respiratory syndrome antibodies in blood donors and slaughterhouse workers in Jeddah and Makkah, Saudi Arabia, fall 2012. J. Infect. Dis. 2014;209:243–246. - PMC - PubMed
-
- Agnihothram S., Yount B.L., Jr., Donaldson E.F., Huynh J., Menachery V.D., Gralinski L.E., Graham R.L., Becker M.M., Tomar S., Scobey T.D., Osswald H.L., Whitmore A., Gopal R., Ghosh A.K., Mesecar A., Zambon M., Heise M., Denison M.R., Baric R.S. A mouse model for Betacoronavirus subgroup 2c using a bat coronavirus strain HKU5 variant. MBio. 2014;5 e00047-14. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
