

Prehospital use of magnesium sulfate as neuroprotection in acute stroke
- PMID: 25651247
- PMCID: PMC4920545
- DOI: 10.1056/NEJMoa1408827
Prehospital use of magnesium sulfate as neuroprotection in acute stroke
Abstract
Background: Magnesium sulfate is neuroprotective in preclinical models of stroke and has shown signals of potential efficacy with an acceptable safety profile when delivered early after stroke onset in humans. Delayed initiation of neuroprotective agents has hindered earlier phase 3 trials of neuroprotective agents.
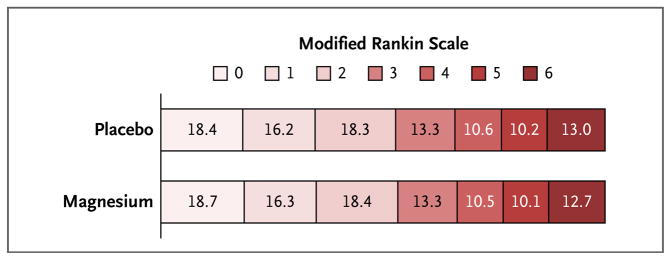
Methods: We randomly assigned patients with suspected stroke to receive either intravenous magnesium sulfate or placebo, beginning within 2 hours after symptom onset. A loading dose was initiated by paramedics before the patient arrived at the hospital, and a 24-hour maintenance infusion was started on the patient's arrival at the hospital. The primary outcome was the degree of disability at 90 days, as measured by scores on the modified Rankin scale (range, 0 to 6, with higher scores indicating greater disability).
Results: Among the 1700 enrolled patients (857 in the magnesium group and 843 in the placebo group), the mean (±SD) age was 69±13 years, 42.6% were women, and the mean pretreatment score on the Los Angeles Motor Scale of stroke severity (range, 0 to 10, with higher scores indicating greater motor deficits) was 3.7±1.3. The final diagnosis of the qualifying event was cerebral ischemia in 73.3% of patients, intracranial hemorrhage in 22.8%, and a stroke-mimicking condition in 3.9%. The median interval between the time the patient was last known to be free of stroke symptoms and the start of the study-drug infusion was 45 minutes (interquartile range, 35 to 62), and 74.3% of patients received the study-drug infusion within the first hour after symptom onset. There was no significant shift in the distribution of 90-day disability outcomes on the global modified Rankin scale between patients in the magnesium group and those in the placebo group (P=0.28 by the Cochran-Mantel-Haenszel test); mean scores at 90 days did not differ between the magnesium group and the placebo group (2.7 in each group, P=1.00). No significant between-group differences were noted with respect to mortality (15.4% in the magnesium group and 15.5% in the placebo group, P=0.95) or all serious adverse events.
Conclusions: Prehospital initiation of magnesium sulfate therapy was safe and allowed the start of therapy within 2 hours after the onset of stroke symptoms, but it did not improve disability outcomes at 90 days. (Funded by the National Institute of Neurological Disorders and Stroke; FAST-MAG ClinicalTrials.gov number, NCT00059332.).
Figures
Similar articles
-
Prehospital neuroprotective therapy for acute stroke: results of the Field Administration of Stroke Therapy-Magnesium (FAST-MAG) pilot trial.Stroke. 2004 May;35(5):e106-8. doi: 10.1161/01.STR.0000124458.98123.52. Epub 2004 Mar 11. Stroke. 2004. PMID: 15017009 Clinical Trial.
-
NXY-059 for acute ischemic stroke.N Engl J Med. 2006 Feb 9;354(6):588-600. doi: 10.1056/NEJMoa052980. N Engl J Med. 2006. PMID: 16467546 Clinical Trial.
-
Magnesium Sulfate and Hematoma Expansion: An Ancillary Analysis of the FAST-MAG Randomized Trial.Stroke. 2022 May;53(5):1516-1519. doi: 10.1161/STROKEAHA.121.037999. Epub 2022 Apr 5. Stroke. 2022. PMID: 35380053 Free PMC article. Clinical Trial.
-
Magnesium neuroprotection is limited in humans with acute brain injury.Neurocrit Care. 2005;2(3):342-51. doi: 10.1385/NCC:2:3:342. Neurocrit Care. 2005. PMID: 16159086 Review.
-
Neuroprotection as initial therapy in acute stroke. Third Report of an Ad Hoc Consensus Group Meeting. The European Ad Hoc Consensus Group.Cerebrovasc Dis. 1998 Jan-Feb;8(1):59-72. doi: 10.1159/000015817. Cerebrovasc Dis. 1998. PMID: 9645985 Review.
Cited by
-
Evolution and Future of Stroke Trials.Stroke. 2024 Jul;55(7):1932-1939. doi: 10.1161/STROKEAHA.123.044265. Epub 2024 Feb 8. Stroke. 2024. PMID: 38328974 Review. No abstract available.
-
Anti-inflammatory and Neuroprotective Agents in Clinical Trials for CNS Disease and Injury: Where Do We Go From Here?Front Immunol. 2020 Sep 10;11:2021. doi: 10.3389/fimmu.2020.02021. eCollection 2020. Front Immunol. 2020. PMID: 33013859 Free PMC article. Review.
-
Dodecafluoropentane Improves Neurological Function Following Anterior Ischemic Stroke.Mol Neurobiol. 2017 Aug;54(6):4764-4770. doi: 10.1007/s12035-016-0019-8. Epub 2016 Aug 8. Mol Neurobiol. 2017. PMID: 27501802 Free PMC article.
-
Prehospital systolic blood pressure is higher in acute stroke compared with stroke mimics.Neurology. 2016 Jun 7;86(23):2146-53. doi: 10.1212/WNL.0000000000002747. Epub 2016 May 18. Neurology. 2016. PMID: 27194383 Free PMC article.
-
Beyond the Golden Hour: Treating Acute Stroke in the Platinum 30 Minutes.Stroke. 2022 Aug;53(8):2426-2434. doi: 10.1161/STROKEAHA.121.036993. Epub 2022 May 12. Stroke. 2022. PMID: 35545939 Free PMC article.
References
-
- Saver JL. Improving reperfusion therapy for acute ischaemic stroke. J Thromb Haemost. 2011;9(Suppl 1):333–43. - PubMed
-
- Saver JL, Jahan R, Levy EI, et al. Solitaire flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel-group, non-inferiority trial. Lancet. 2012;380:1241–9. - PubMed
-
- Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. - PubMed
-
- Kidwell CS, Liebeskind DS, Starkman S, Saver JL. Trends in acute ischemic stroke trials through the 20th century. Stroke. 2001;32:1349–59. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials