

Cytokines in psoriasis
- PMID: 25585875
- PMCID: PMC4437803
- DOI: 10.1016/j.cyto.2014.12.014
Cytokines in psoriasis
Abstract
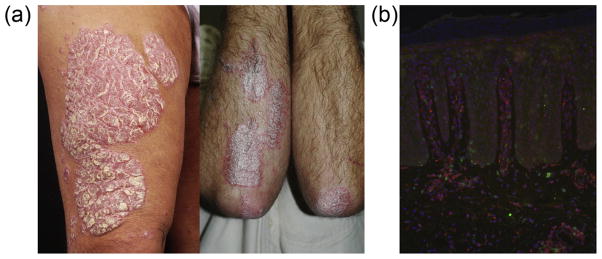
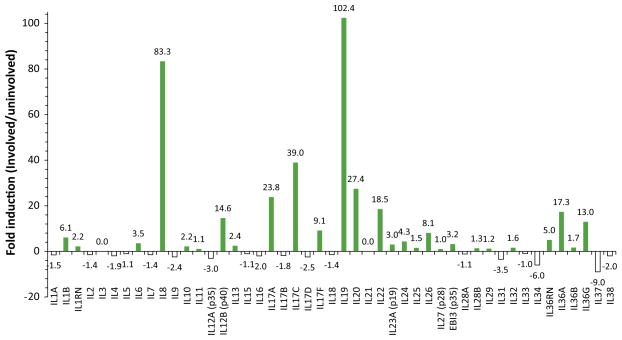
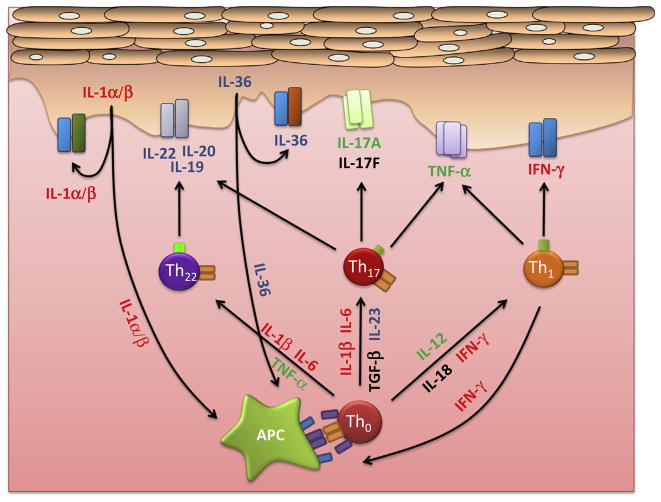
Psoriasis is a common inflammatory skin disease with an incompletely understood etiology. The disease is characterized by red, scaly and well-demarcated skin lesions formed by the hyperproliferation of epidermal keratinocytes. This hyperproliferation is driven by cytokines secreted by activated resident immune cells, an infiltrate of T cells, dendritic cells and cells of the innate immune system, as well as the keratinocytes themselves. Psoriasis has a strong hereditary character and has a complex genetic background. Genome-wide association studies have identified polymorphisms within or near a number of genes encoding cytokines, cytokine receptors or elements of their signal transduction pathways, further implicating these cytokines in the psoriasis pathomechanism. A considerable number of inflammatory cytokines have been shown to be elevated in lesional psoriasis skin, and the serum concentrations of a subset of these also correlate with psoriasis disease severity. The combined effects of the cytokines found in psoriasis lesions likely explain most of the clinical features of psoriasis, such as the hyperproliferation of keratinocytes, increased neovascularization and skin inflammation. Thus, understanding which cytokines play a pivotal role in the disease process can suggest potential therapeutic targets. A number of cytokines have been therapeutically targeted with success, revolutionizing treatment of this disease. Here we review a number of key cytokines implicated in the pathogenesis of psoriasis.
Keywords: Cytokine; Inflammation; Interleukin; Psoriasis; Skin.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Etiology and Pathogenesis of Psoriasis.Rheum Dis Clin North Am. 2015 Nov;41(4):665-75. doi: 10.1016/j.rdc.2015.07.013. Epub 2015 Sep 5. Rheum Dis Clin North Am. 2015. PMID: 26476225 Review.
-
T lymphocytes derived from skin lesions of patients with psoriasis vulgaris express a novel cytokine pattern that is distinct from that of T helper type 1 and T helper type 2 cells.Eur J Immunol. 1994 Oct;24(10):2377-82. doi: 10.1002/eji.1830241018. Eur J Immunol. 1994. PMID: 7925564
-
Resident skin cells in psoriasis: a special look at the pathogenetic functions of keratinocytes.Clin Dermatol. 2007 Nov-Dec;25(6):581-8. doi: 10.1016/j.clindermatol.2007.08.013. Clin Dermatol. 2007. PMID: 18021896 Review.
-
Molecular pathophysiology of psoriasis and molecular targets of antipsoriatic therapy.Expert Rev Mol Med. 2009 Dec 14;11:e38. doi: 10.1017/S146239940900129X. Expert Rev Mol Med. 2009. PMID: 20003607
-
[The role of perforin mediated cell cytotoxicity in psoriasis].Lijec Vjesn. 2010 Nov-Dec;132(11-12):361-4. Lijec Vjesn. 2010. PMID: 21294326 Review. Croatian.
Cited by
-
Ebosin Ameliorates Psoriasis-Like Inflammation of Mice via miR-155 Targeting tnfaip3 on IL-17 Pathway.Front Immunol. 2021 Apr 26;12:662362. doi: 10.3389/fimmu.2021.662362. eCollection 2021. Front Immunol. 2021. PMID: 33981308 Free PMC article.
-
Chemokine Profile in Psoriasis Patients in Correlation with Disease Severity and Pruritus.Int J Mol Sci. 2022 Nov 1;23(21):13330. doi: 10.3390/ijms232113330. Int J Mol Sci. 2022. PMID: 36362116 Free PMC article.
-
The Skin Reservoir Model: A Tool for Evaluating Microdialysis Sampling of Large Biomarkers from Human Skin.Acta Derm Venereol. 2020 Jan 7;100(1):adv00008. doi: 10.2340/00015555-3356. Acta Derm Venereol. 2020. PMID: 31626324 Free PMC article.
-
Genistein-Opportunities Related to an Interesting Molecule of Natural Origin.Molecules. 2022 Jan 26;27(3):815. doi: 10.3390/molecules27030815. Molecules. 2022. PMID: 35164079 Free PMC article. Review.
-
Psoriasis, Cardiovascular Events, and Biologics: Lights and Shadows.Front Immunol. 2018 Aug 13;9:1668. doi: 10.3389/fimmu.2018.01668. eCollection 2018. Front Immunol. 2018. PMID: 30150978 Free PMC article. Review.
References
-
- Parisi R, Symmons DP, Griffiths CE, Ashcroft DM. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2012 - PubMed
-
- Di Cesare A, Di Meglio P, Nestle FO. The IL-23/Th17 axis in the immunopathogenesis of psoriasis. J Invest Dermatol. 2009;129:1339–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
