

A detailed clinicopathologic study of ALK-translocated papillary thyroid carcinoma
- PMID: 25501013
- PMCID: PMC4415964
- DOI: 10.1097/PAS.0000000000000368
A detailed clinicopathologic study of ALK-translocated papillary thyroid carcinoma
Abstract
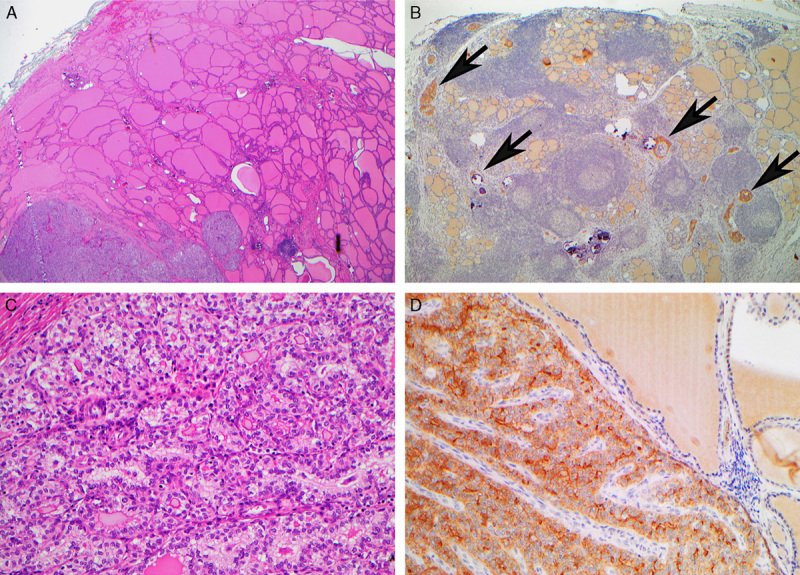
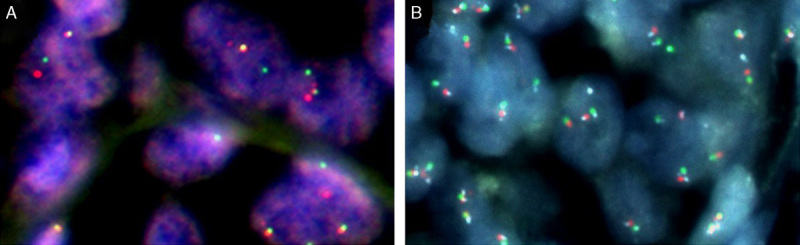
Pathogenic ALK translocations have been reported in papillary thyroid carcinoma (PTC). We developed and validated a screening algorithm based on immunohistochemistry (IHC), followed by fluorescence in situ hybridization (FISH) in IHC-positive cases to identify ALK-rearranged PTC. IHC and FISH were performed in a cohort of 259 thyroid carcinomas enriched for aggressive variants. IHC was positive in 8 cases, 6 confirmed translocated by FISH (specificity 75%). All 251 IHC-negative cases were FISH negative (sensitivity 100%). Having validated this approach, we performed screening IHC, followed by FISH in IHC-positive cases in an expanded cohort. ALK translocations were identified in 11 of 498 (2.2%) of all consecutive unselected PTCs and 3 of 23 (13%) patients with diffuse sclerosing variant PTCs. No ALK translocations were identified in 36 PTCs with distant metastases, 28 poorly differentiated (insular) carcinomas, and 20 anaplastic carcinomas. All 14 patients with ALK translocations were female (P=0.0425), and translocations occurred at a younger age (mean 38 vs. 48 y, P=0.0289 in unselected patients). ALK translocation was an early clonal event present in all neoplastic cells and mutually exclusive with BRAF mutation. ALK translocation was not associated with aggressive clinicopathologic features (size, stage, metastasis, vascular invasion, extrathyroidal extension, multifocality, risk for recurrence, radioiodine resistance). We conclude that 2.2% of PTCs are ALK-translocated and can be identified by screening IHC followed by FISH. ALK translocations may be more common in young females and diffuse sclerosing variant PTC but do not connote more aggressive disease.
Conflict of interest statement
Conflicts of Interest and Source of Funding: Supported by the Cancer Institute NSW through the Sydney Vital Translational Research Centre. S.O.T. and A.J.G. report receiving honoraria from lectures from Pfizer, manufacturers of crizotinib. S.O.T. was also supported by the Sydney Breast Cancer Foundation for this study. For the remaining authors none were declared.
Figures

Similar articles
-
Clinicopathological features and immunohistochemical utility of NTRK-, ALK-, and ROS1-rearranged papillary thyroid carcinomas and anaplastic thyroid carcinomas.Hum Pathol. 2020 Dec;106:82-92. doi: 10.1016/j.humpath.2020.09.004. Epub 2020 Sep 25. Hum Pathol. 2020. PMID: 32980422
-
Clinicopathologic correlations of the BRAFV600E mutation, BRAF V600E immunohistochemistry, and BRAF RNA in situ hybridization in papillary thyroid carcinoma.Pathol Res Pract. 2015 Feb;211(2):162-70. doi: 10.1016/j.prp.2014.10.005. Epub 2014 Oct 27. Pathol Res Pract. 2015. PMID: 25468810
-
Anaplastic lymphoma kinase (ALK) gene rearrangements in radiation-related human papillary thyroid carcinoma after the Chernobyl accident.J Pathol Clin Res. 2018 Jul;4(3):175-183. doi: 10.1002/cjp2.102. Epub 2018 May 26. J Pathol Clin Res. 2018. PMID: 29633575 Free PMC article.
-
Cytologic, clinicopathologic, and molecular features of papillary thyroid carcinoma with prominent hobnail features: 10 case reports and systematic literature review.Int J Clin Exp Pathol. 2015 Jul 1;8(7):7988-97. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 26339365 Free PMC article. Review.
-
Evidence that one subset of anaplastic thyroid carcinomas are derived from papillary carcinomas due to BRAF and p53 mutations.Cancer. 2005 Jun 1;103(11):2261-8. doi: 10.1002/cncr.21073. Cancer. 2005. PMID: 15880523 Review.
Cited by
-
Combinatorial Therapies in Thyroid Cancer: An Overview of Preclinical and Clinical Progresses.Cells. 2020 Mar 30;9(4):830. doi: 10.3390/cells9040830. Cells. 2020. PMID: 32235612 Free PMC article. Review.
-
Antineoplastic Effect of ALK Inhibitor Crizotinib in Primary Human Anaplastic Thyroid Cancer Cells with STRN-ALK Fusion In Vitro.Int J Mol Sci. 2024 Jun 19;25(12):6734. doi: 10.3390/ijms25126734. Int J Mol Sci. 2024. PMID: 38928438 Free PMC article.
-
Novel targeted therapies and immunotherapy for advanced thyroid cancers.Mol Cancer. 2018 Feb 19;17(1):51. doi: 10.1186/s12943-018-0786-0. Mol Cancer. 2018. PMID: 29455653 Free PMC article. Review.
-
Anaplastic lymphoma kinase inhibitors-a review of anticancer properties, clinical efficacy, and resistance mechanisms.Front Pharmacol. 2023 Oct 25;14:1285374. doi: 10.3389/fphar.2023.1285374. eCollection 2023. Front Pharmacol. 2023. PMID: 37954850 Free PMC article. Review.
-
Inhibition of ALK-Signaling Overcomes STRN-ALK-Induced Downregulation of the Sodium Iodine Symporter and Restores Radioiodine Uptake in Thyroid Cells.Thyroid. 2023 Apr;33(4):464-473. doi: 10.1089/thy.2022.0533. Epub 2023 Feb 27. Thyroid. 2023. PMID: 36585857 Free PMC article.
References
-
- Davies L, Welch G. Increasing Incidence of Thyroid Cancer in the United States, 1973-2002. JAMA. 2006;295:2164–2167. - PubMed
-
- Gonzalez-Gonzalez R, Bologna-Molina R, Carreon-Burciaga RG, et al. Papillary Thyroid Carcinoma: Differential Diagnosis and Prognostic Values of Its Different Variants: Review of the Literature. ISRN Oncology 2011;2011:915925. doi:10.5402/2011/915925. - DOI - PMC - PubMed
-
- DeLellis RA, Lloyd RV, Heitz PU, et al. World Health Organization Classification of Tumours: Pathology and Genetics of Tumours of Endocrine Organs. 2004Lyon, France:IARC Press;51–80.
-
- Hay ID, Thompson GB, Grant CS, et al. Papillary thyroid carcinoma managed at the Mayo Clinic during six decades (1940-1999): temporal trends in initial therapy and long-term outcome in 2444 consecutively treated patients. World J Surg. 2002;26:879–885. - PubMed
-
- Nixon I, Ganly I, Patel SG, et al. Changing trends in well differentiated thyroid carcinoma over eight decades. Int J Surg. 2012;10:618–623. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
