

A new paradigm: Diagnosis and management of HSCT-associated thrombotic microangiopathy as multi-system endothelial injury
- PMID: 25483393
- PMCID: PMC4659438
- DOI: 10.1016/j.blre.2014.11.001
A new paradigm: Diagnosis and management of HSCT-associated thrombotic microangiopathy as multi-system endothelial injury
Abstract
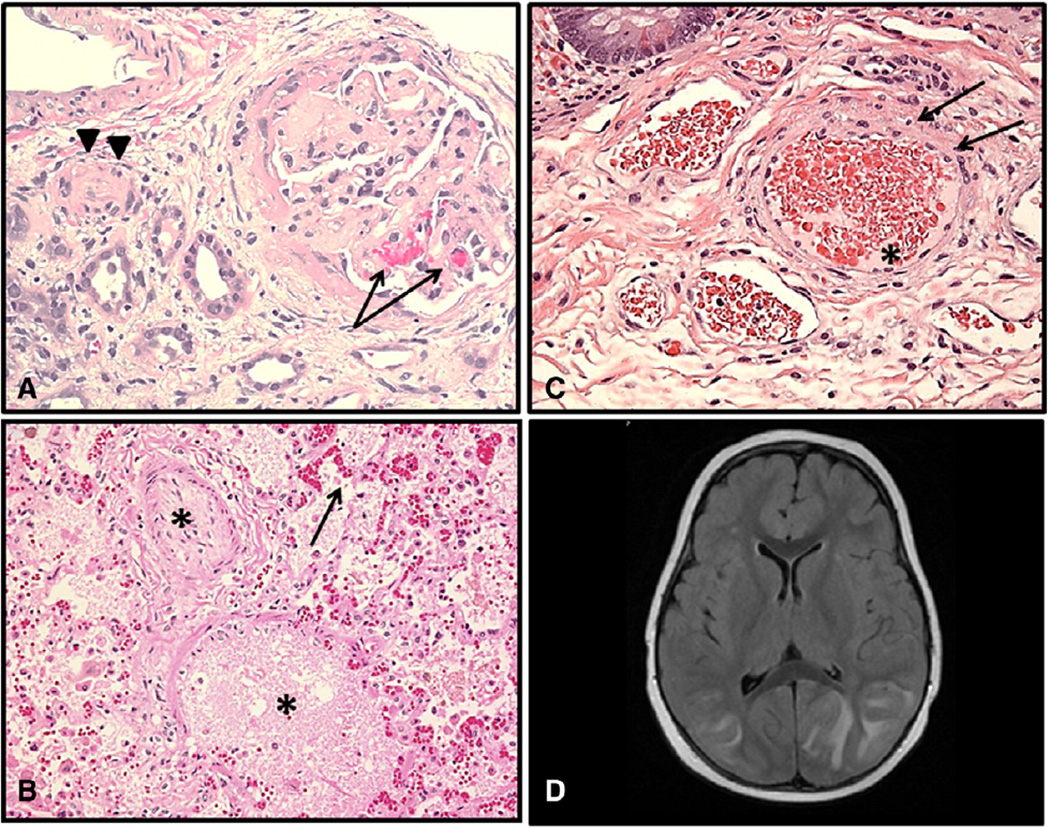
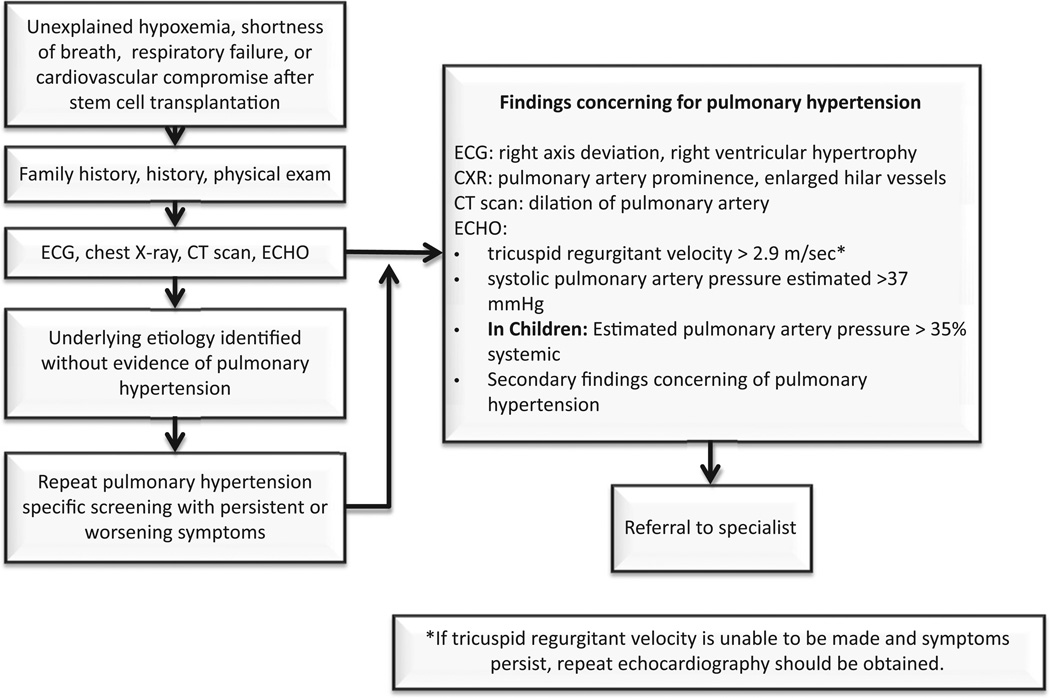
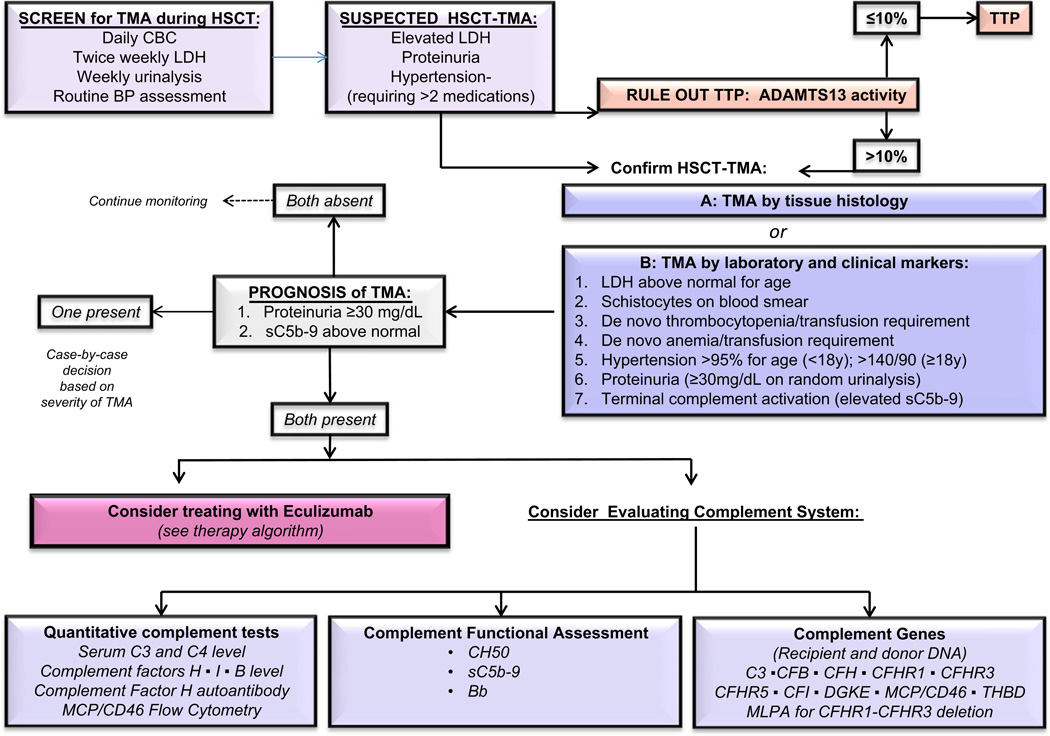
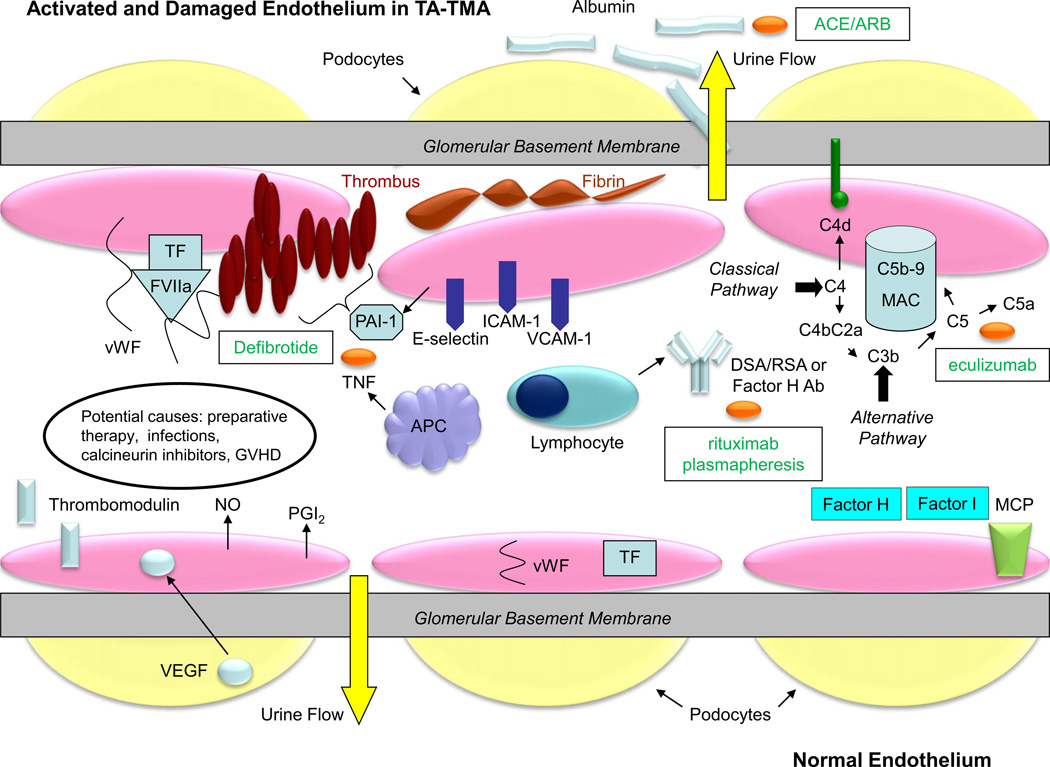
Hematopoietic stem cell transplantation (HSCT)-associated thrombotic microangiopathy (TA-TMA) is now a well-recognized and potentially severe complication of HSCT that carries a high risk of death. In those who survive, TA-TMA may be associated with long-term morbidity and chronic organ injury. Recently, there have been new insights into the incidence, pathophysiology, and management of TA-TMA. Specifically, TA-TMA can manifest as a multi-system disease occurring after various triggers of small vessel endothelial injury, leading to subsequent tissue damage in different organs. While the kidney is most commonly affected, TA-TMA involving organs such as the lung, bowel, heart, and brain is now known to have specific clinical presentations. We now review the most up-to-date research on TA-TMA, focusing on the pathogenesis of endothelial injury, the diagnosis of TA-TMA affecting the kidney and other organs, and new clinical approaches to the management of this complication after HSCT.
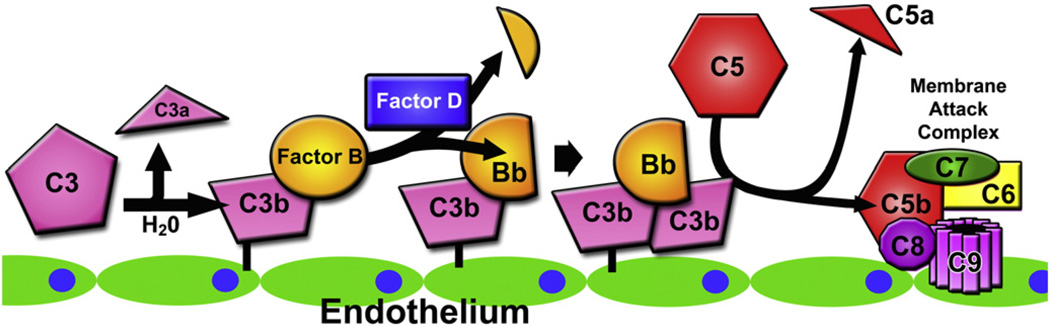
Keywords: Complement activation; Eculizumab; Hematopoietic cell transplant; Kidney disease; TA-TMA; Thrombotic microangiopathy.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
BPD serves on the speaker’s bureau and as a consultant for Alexion Pharmaceuticals. SJ and BLL are co-inventors of a patent application: “Compositions and Methods for Treatment of HSCT-Associated Thrombotic Microangiopathy” (application number PCT/US2014/055922). CED, MCM,JE, SMD,JG have no financial disclosures.
Figures
Similar articles
-
New approaches in the diagnosis, pathophysiology, and treatment of pediatric hematopoietic stem cell transplantation-associated thrombotic microangiopathy.Transfus Apher Sci. 2016 Apr;54(2):181-90. doi: 10.1016/j.transci.2016.04.007. Epub 2016 Apr 25. Transfus Apher Sci. 2016. PMID: 27156964 Free PMC article. Review.
-
Emerging Concepts in Hematopoietic Stem Cell Transplantation-Associated Renal Thrombotic Microangiopathy and Prospects for New Treatments.Am J Kidney Dis. 2018 Dec;72(6):857-865. doi: 10.1053/j.ajkd.2018.06.013. Epub 2018 Aug 23. Am J Kidney Dis. 2018. PMID: 30146419 Review.
-
Hematopoietic stem cell transplant-associated thrombotic microangiopathy: review of pharmacologic treatment options.Transfusion. 2015 Feb;55(2):452-8. doi: 10.1111/trf.12859. Epub 2014 Sep 11. Transfusion. 2015. PMID: 25209960 Review.
-
The alternative complement pathway activation product Ba as a marker for transplant-associated thrombotic microangiopathy.Pediatr Blood Cancer. 2020 Mar;67(3):e28070. doi: 10.1002/pbc.28070. Epub 2019 Nov 27. Pediatr Blood Cancer. 2020. PMID: 31774252
-
Neurological involvement in hematopoietic stem cell transplantation-associated thrombotic microangiopathy.Ann Hematol. 2024 Sep;103(9):3303-3313. doi: 10.1007/s00277-024-05798-6. Epub 2024 May 20. Ann Hematol. 2024. PMID: 38763940 Free PMC article. Review.
Cited by
-
Where have all the platelets gone? HIT, DIC, or something else?Hematology Am Soc Hematol Educ Program. 2023 Dec 8;2023(1):43-50. doi: 10.1182/hematology.2023000465. Hematology Am Soc Hematol Educ Program. 2023. PMID: 38066886 Free PMC article. Review.
-
New approaches in the diagnosis, pathophysiology, and treatment of pediatric hematopoietic stem cell transplantation-associated thrombotic microangiopathy.Transfus Apher Sci. 2016 Apr;54(2):181-90. doi: 10.1016/j.transci.2016.04.007. Epub 2016 Apr 25. Transfus Apher Sci. 2016. PMID: 27156964 Free PMC article. Review.
-
Transplant-associated thrombotic microangiopathy in pediatric patients: pre-HSCT risk stratification and prophylaxis.Blood Adv. 2021 Apr 27;5(8):2106-2114. doi: 10.1182/bloodadvances.2020003988. Blood Adv. 2021. PMID: 33877298 Free PMC article.
-
COVID-19 infection in paediatric recipients of allogeneic stem cell transplantation: the UK experience.Br J Haematol. 2021 Aug;194(4):e74-e77. doi: 10.1111/bjh.17547. Epub 2021 Jun 20. Br J Haematol. 2021. PMID: 34132400 Free PMC article. No abstract available.
-
Case report: Thrombotic microangiopathy concomitant with macrophage activation syndrome in systemic lupus erythematosus refractory to conventional treatment successfully treated with eculizumab.Front Med (Lausanne). 2023 Jan 9;9:1097528. doi: 10.3389/fmed.2022.1097528. eCollection 2022. Front Med (Lausanne). 2023. PMID: 36698804 Free PMC article.
References
-
- George JN, Li X, McMinn JR, Terrell DR, Vesely SK, Selby GB. Thrombotic thrombocytopenic purpura-hemolytic uremic syndrome following allogeneic HPC transplantation: a diagnostic dilemma. Transfusion. 2004;44:294–304. - PubMed
-
- Kersting S, Koomans HA, Hene RJ, Verdonck LF. Acute renal failure after allogeneic myeloablative stem cell transplantation: retrospective analysis of incidence, risk factors and survival. Bone Marrow Transplant. 2007;39:359–365. - PubMed
-
- Parikh CR, McSweeney P, Schrier RW. Acute renal failure independently predicts mortality after myeloablative allogeneic hematopoietic cell transplant. Kidney Int. 2005;67:1999–2005. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
