

Congenital upper eyelid coloboma: embryologic, nomenclatorial, nosologic, etiologic, pathogenetic, epidemiologic, clinical, and management perspectives
- PMID: 25419956
- PMCID: PMC4334304
- DOI: 10.1097/IOP.0000000000000347
Congenital upper eyelid coloboma: embryologic, nomenclatorial, nosologic, etiologic, pathogenetic, epidemiologic, clinical, and management perspectives
Abstract
Purpose: To review the recent literature and describe the authors' experience with congenital upper eyelid coloboma.
Methods: In this review, we will summarize the embryologic and etiopathogenetic bases of congenital upper eyelid coloboma, and study the published clinical reports. We will also attempt to briefly shed some light on the rarer syndromic curiosities associated with upper eyelid coloboma.
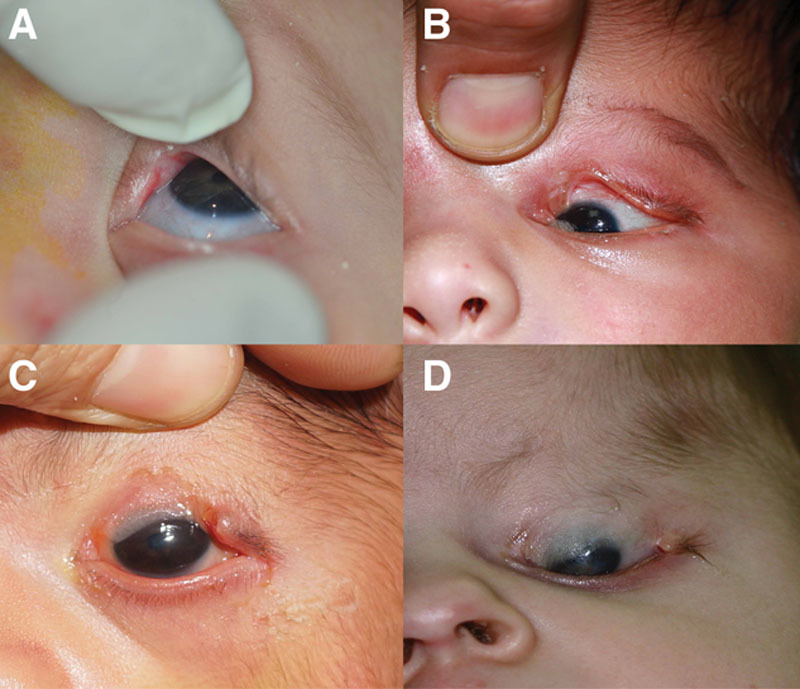
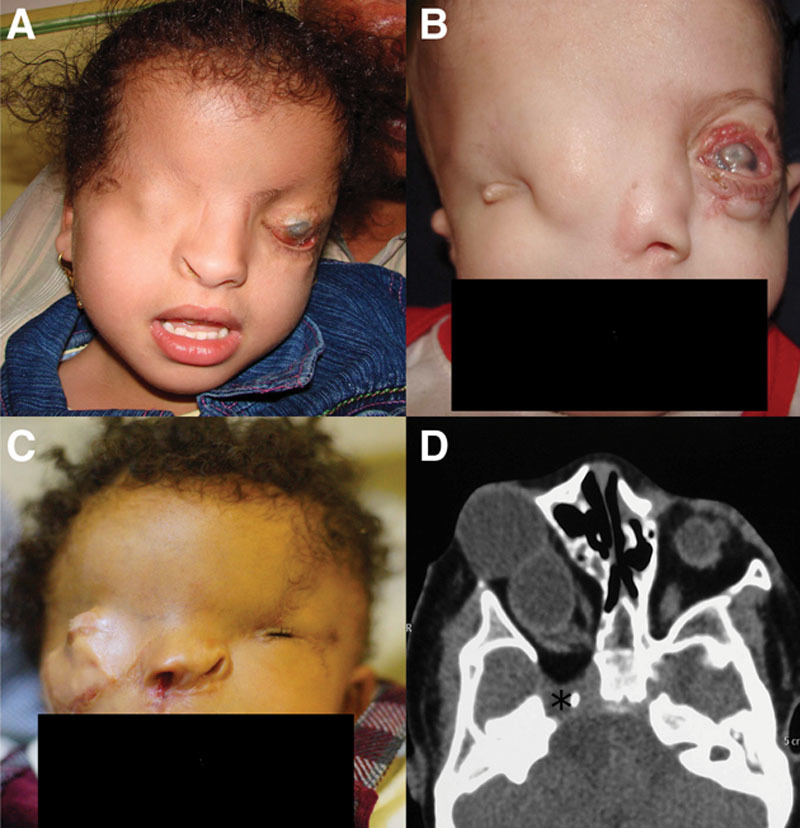
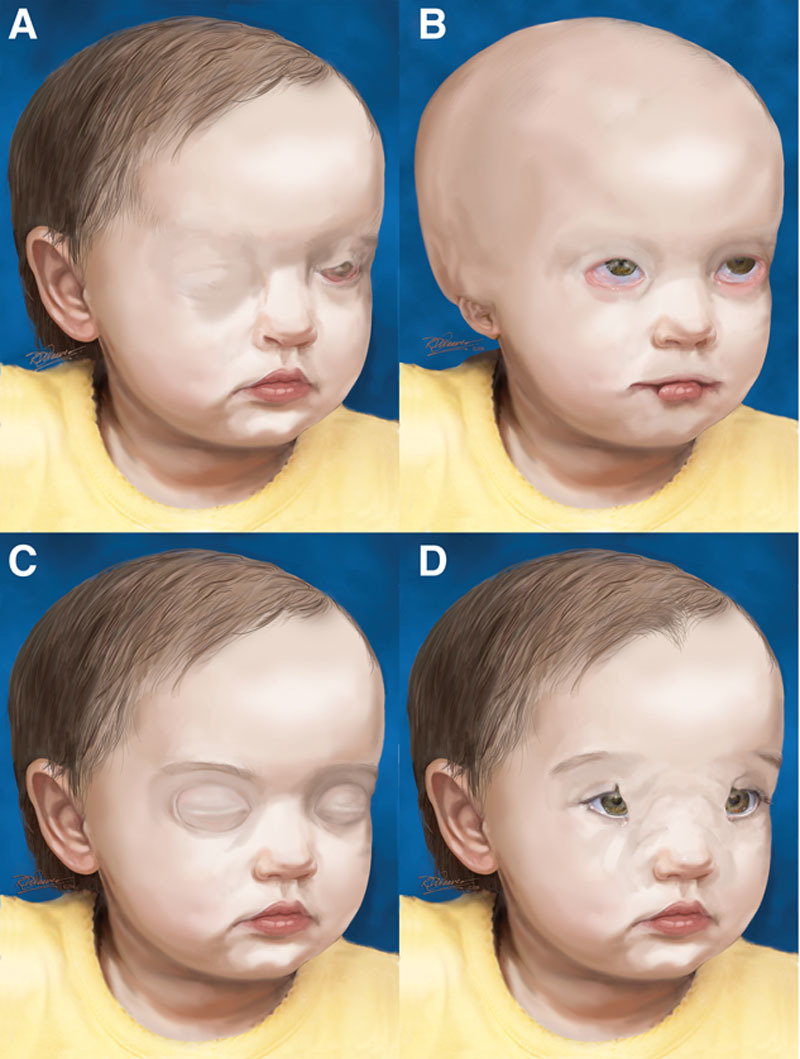
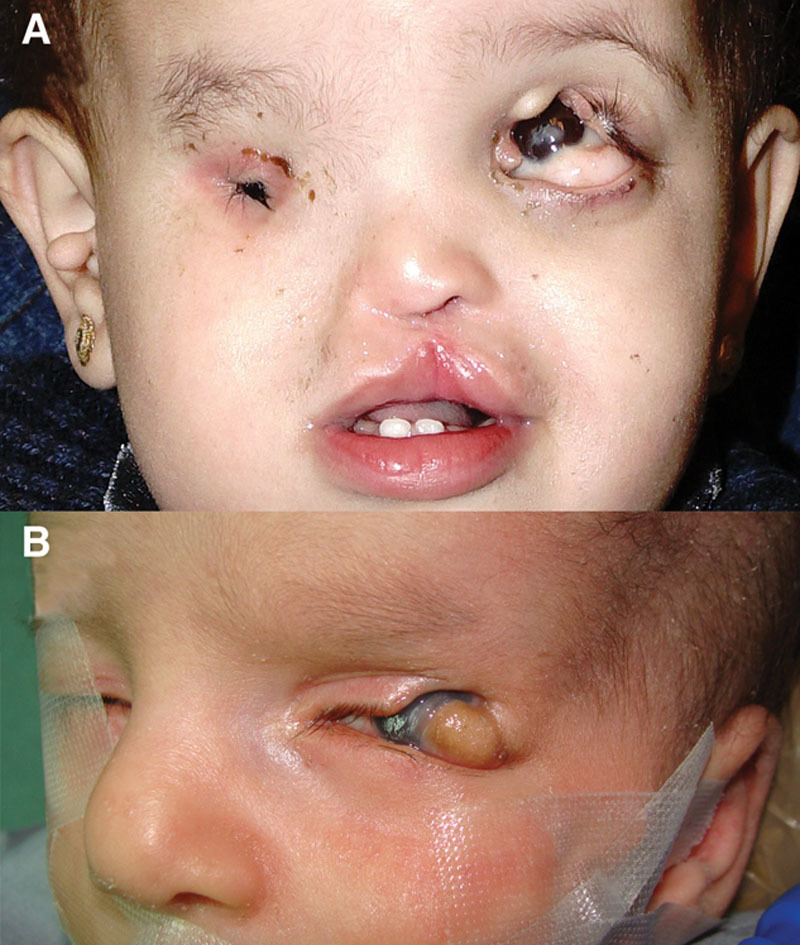
Results: Congenital upper eyelid colobomas are one of the few nontraumatic oculoplastic emergencies that may occasionally present in the first few days of life with a corneal ulcer and may even present with impending perforation. They can present with or without corneopalpebral adhesions, may be isolated findings or a part of a larger spectrum of congenital anomalies as in the case of Fraser syndrome or Goldenhar syndrome, or could be associated with other rare curiosities that could challenge the clinician with a huge diagnostic dilemma.
Conclusions: Existing literature dealing with congenital colobomas of the upper eyelid is fraught with nosologic problems, confusing etiologies, and overlapping clinical features. We attempted to clarify the salient clinical features, outline the management principles, and until a time in the not-so-distant future where advances in molecular genetic testing would help redefine the etiology and the diverse clinical spectrum of genetic diseases associated with upper eyelid colobomas, we propose a simplified classification scheme based on the relation of the coloboma to the cornea, the presence or absence of systemic features, and all the syndromic and nonsyndromic associations of congenital coloboma of the upper eyelid known today.
Conflict of interest statement
The authors have no financial or conflicts of interest in the study.
Figures


Similar articles
-
Congenital eyelid colobomas in 51 patients.J Pediatr Ophthalmol Strabismus. 2009 May-Jun;46(3):151-9. doi: 10.3928/01913913-20090505-06. J Pediatr Ophthalmol Strabismus. 2009. PMID: 19496496
-
Congenital upper lid colobomas: management and visual outcome.Ophthalmic Plast Reconstr Surg. 2002 May;18(3):190-5. doi: 10.1097/00002341-200205000-00007. Ophthalmic Plast Reconstr Surg. 2002. PMID: 12021649
-
Tarsomarginal graft in upper eyelid coloboma repair.J AAPOS. 2007 Oct;11(5):499-501. doi: 10.1016/j.jaapos.2007.04.011. Epub 2007 Jul 19. J AAPOS. 2007. PMID: 17644442
-
State of the Art in Congenital Eyelid Deformity Management.Facial Plast Surg. 2016 Apr;32(2):142-9. doi: 10.1055/s-0036-1581049. Epub 2016 Apr 20. Facial Plast Surg. 2016. PMID: 27097135 Review.
-
Surgery of the eyelids.Clin Plast Surg. 1998 Oct;25(4):579-86, ix. Clin Plast Surg. 1998. PMID: 9917977 Review.
Cited by
-
Eyelid and fornix reconstruction in abortive cryptophthalmos: a single-center experience over 12 years.Eye (Lond). 2017 Nov;31(11):1576-1581. doi: 10.1038/eye.2017.94. Epub 2017 Jun 16. Eye (Lond). 2017. PMID: 28622309 Free PMC article.
-
Congenital Eyelid Anomalies: What General Physicians Need To Know.Oman Med J. 2021 Jul 6;36(4):e279. doi: 10.5001/omj.2021.26. eCollection 2021 Jul. Oman Med J. 2021. PMID: 34267952 Free PMC article. Review.
-
A 5-day-old-newborn with a large right upper eyelid coloboma.Digit J Ophthalmol. 2017 Sep 28;23(3):88-91. doi: 10.5693/djo.03.2017.08.001. eCollection 2017. Digit J Ophthalmol. 2017. PMID: 29162995 Free PMC article. No abstract available.
-
Embryologic and Fetal Development of the Human Eyelid.Ophthalmic Plast Reconstr Surg. 2016 Nov/Dec;32(6):407-414. doi: 10.1097/IOP.0000000000000702. Ophthalmic Plast Reconstr Surg. 2016. PMID: 27124372 Free PMC article. Review.
-
Ophthalmic features and management outcomes of 30 children having Goldenhar syndrome.Int Ophthalmol. 2020 Mar;40(3):667-675. doi: 10.1007/s10792-019-01227-0. Epub 2019 Nov 23. Int Ophthalmol. 2020. PMID: 31760545
References
-
- Anderson KN, Anderson LE, Glanze WD. In: Mosby’s Medical, Nursing and Allied Health Dictionary. 4th ed. St. Louis: Mosby; 1994. Coloboma. p. 3613.
-
- Dorland WN, Taylor EJ. Dorland’s Illustrated Medical Dictionary. 27th ed. Philadelphia, PA: WB Saunders; 1988. p. 359.
-
- Onwochei BC, Simon JW, Bateman JB, et al. Ocular colobomata. Surv Ophthalmol. 2000;45:175–94. - PubMed
-
- Saleh GM, Hussain B, Verity DH, et al. A surgical strategy for the correction of Fraser syndrome cryptophthalmos. Ophthalmology. 2009;116:1707–12. - PubMed
-
- Pavlakis E, Chiotaki R, Chalepakis G. The role of Fras1/Frem proteins in the structure and function of basement membrane. Int J Biochem Cell Biol. 2011;43:487–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
