

Review
doi: 10.1136/gutjnl-2014-308048.
Epub 2014 Nov 21.
ECM remodelling in IBD: innocent bystander or partner in crime? The emerging role of extracellular molecular events in sustaining intestinal inflammation
Affiliations
- PMID: 25416065
- PMCID: PMC4345769
- DOI: 10.1136/gutjnl-2014-308048
Item in Clipboard
Review
ECM remodelling in IBD: innocent bystander or partner in crime? The emerging role of extracellular molecular events in sustaining intestinal inflammation
Gut.
2015 Mar.
No abstract available
Keywords: EXTRACELLULAR MATRIX; IBD; IBD BASIC RESEARCH; IBD CLINICAL.
Figures
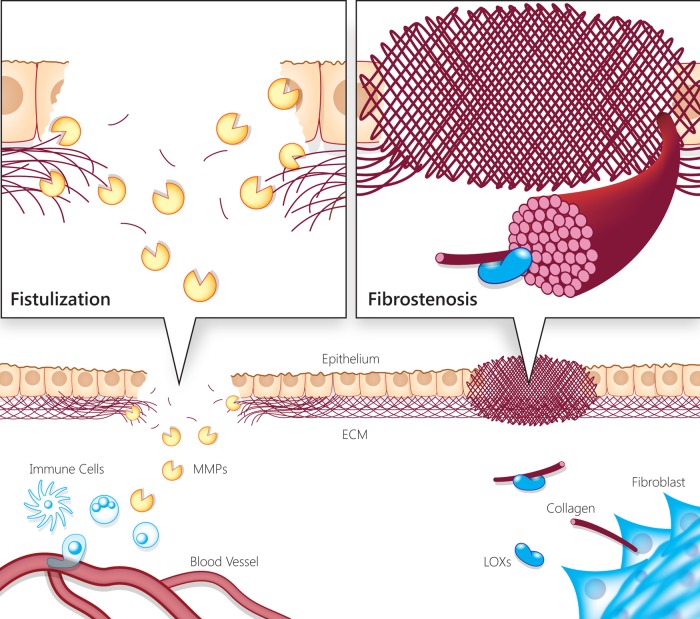
Illustration of IBD-associated progressive tissue damage and complications due to extracellular matrix (ECM) remodelling imbalance and dysregulation. The illustration represents the two faces of progressive tissue damage and complications associated with IBD, resulting from imbalanced and dysregulated ECM remodelling (ie, fistulising vs fibrostenotic disease). During chronic intestinal inflammation, the ECM is remodelled due to secretion of enzymes and structural components by immune, epithelial and stromal cells. Matrix metalloproteinases (MMPs) contribute to epithelial and endothelial barrier disruption and enable immune cells to infiltrate into the tissue. Extracellular proteolysis is a propagator of inflammation via cytokine processing, and release of bioactive molecules from the ECM. On the other hand, fibrotic processes also take place simultaneously by fibroblast activation and secretion of ECM components that assemble via lysyl oxidase (LOX) activity. In turn, the increased stiffness of this fibrotic tissue leads to further fibrogenesis. Therefore, both the destructive and fibrogenic processes in the ECM are self-amplifying and contribute to the tissue damage and excess inflammatory response characteristic of IBD.
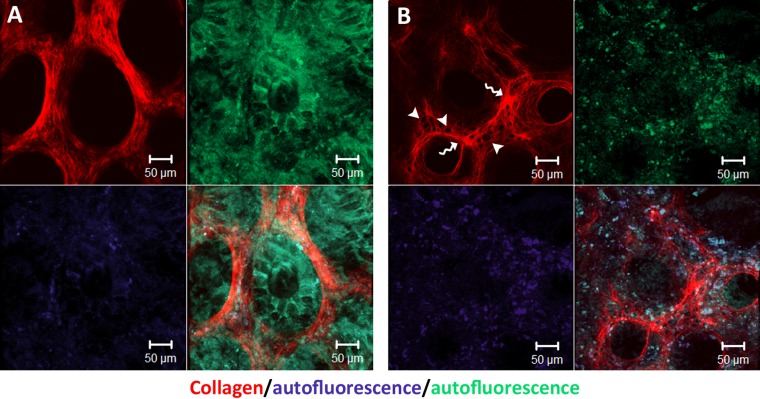
Second-harmonic imaging of native human colon biopsies revealing extracellular matrix (ECM) remodelling in IBD. All samples were thawed in phosphate buffered saline and immediately imaged under two-photon microscope (×20 objective). (A) Healthy colon biopsy from a patient without IBD. (B) Inflamed colon biopsy from a patient with IBD. Note the thickening of ECM barrier between crypts (indicated by curvy arrows), the formation of holes within this barrier (indicated by arrowheads) and changes in collagen microstructure.
Similar articles
-
Role of non-inflammatory factors in intestinal fibrosis.J Dig Dis. 2020 Jun;21(6):315-318. doi: 10.1111/1751-2980.12883. J Dig Dis. 2020. PMID: 32406603 Review.
-
The extracellular matrix in IBD: a dynamic mediator of inflammation.Curr Opin Gastroenterol. 2017 Jul;33(4):234-238. doi: 10.1097/MOG.0000000000000368. Curr Opin Gastroenterol. 2017. PMID: 28562487 Free PMC article. Review.
-
Wound healing and fibrosis in intestinal disease.Gut. 2007 Jan;56(1):130-9. doi: 10.1136/gut.2006.090456. Gut. 2007. PMID: 17172588 Free PMC article. Review. No abstract available.
-
Intestinal Barrier Dysfunction in Human Pathology and Aging.Curr Pharm Des. 2016;22(30):4645-4650. doi: 10.2174/1381612822666160510125331. Curr Pharm Des. 2016. PMID: 27160754 Review.
-
Quantitative assessment of intestinal stiffness and associations with fibrosis in human inflammatory bowel disease.PLoS One. 2018 Jul 11;13(7):e0200377. doi: 10.1371/journal.pone.0200377. eCollection 2018. PLoS One. 2018. PMID: 29995938 Free PMC article.
Cited by
-
Inflammatory Bowel Disease-Associated Gut Commensals Degrade Components of the Extracellular Matrix.mBio. 2022 Dec 20;13(6):e0220122. doi: 10.1128/mbio.02201-22. Epub 2022 Nov 29. mBio. 2022. PMID: 36445085 Free PMC article.
-
Toward Molecular Imaging of Intestinal Pathology.Inflamm Bowel Dis. 2020 Sep 18;26(10):1470-1484. doi: 10.1093/ibd/izaa213. Inflamm Bowel Dis. 2020. PMID: 32793946 Free PMC article. Review.
-
Serological Biomarkers of Tissue Turnover Identify Responders to Anti-TNF Therapy in Crohn's Disease: A Pilot Study.Clin Transl Gastroenterol. 2020 Sep;11(9):e00217. doi: 10.14309/ctg.0000000000000217. Clin Transl Gastroenterol. 2020. PMID: 33094957 Free PMC article.
-
Platelet hyaluronidase-2 regulates the early stages of inflammatory disease in colitis.Blood. 2019 Aug 29;134(9):765-775. doi: 10.1182/blood.2018893594. Epub 2019 Jul 1. Blood. 2019. PMID: 31262781 Free PMC article.
-
Enhanced Collagen Deposition in the Duodenum of Patients with Hyaline Fibromatosis Syndrome and Protein Losing Enteropathy.Int J Mol Sci. 2020 Nov 2;21(21):8200. doi: 10.3390/ijms21218200. Int J Mol Sci. 2020. PMID: 33147779 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources