

Antibodies to myelin oligodendrocyte glycoprotein in bilateral and recurrent optic neuritis
- PMID: 25364774
- PMCID: PMC4215392
- DOI: 10.1212/NXI.0000000000000040
Antibodies to myelin oligodendrocyte glycoprotein in bilateral and recurrent optic neuritis
Abstract
Objective: We examined a cohort of adults with aquaporin-4 (AQP4) antibody-negative neuromyelitis optica/neuromyelitis optica spectrum disorder (NMO/NMOSD) for antibodies to myelin oligodendrocyte glycoprotein (MOG).
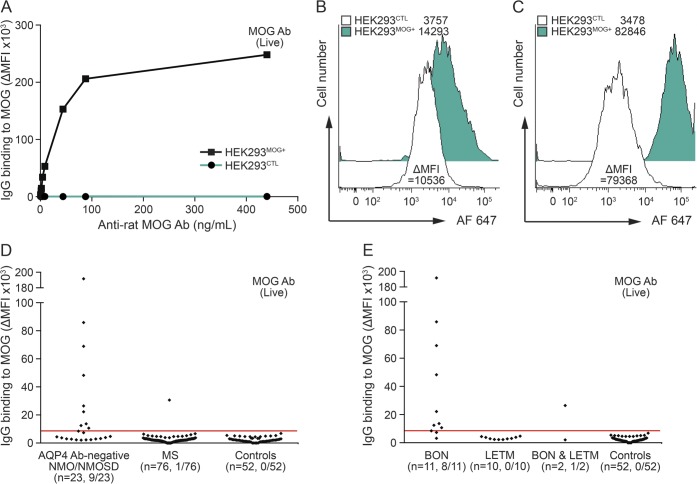
Methods: We performed a flow cytometry cell-based assay using live human lentivirus-transduced cells expressing full-length surface MOG. Serum was tested in 23 AQP4 antibody-negative NMO/NMOSD patients with bilateral and/or recurrent optic neuritis (BON, n = 11), longitudinally extensive transverse myelitis (LETM, n = 10), and sequential BON and LETM (n = 2), as well as in patients with multiple sclerosis (MS, n = 76) and controls (n = 52).
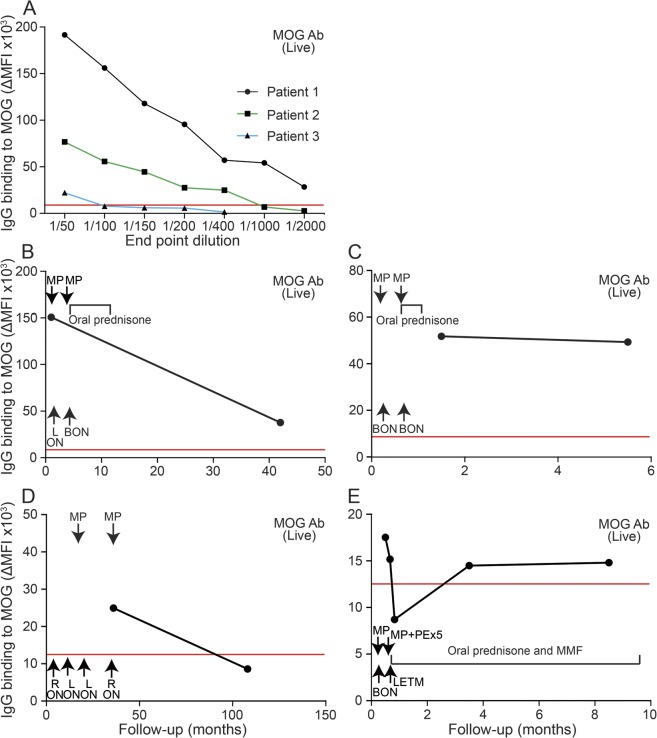
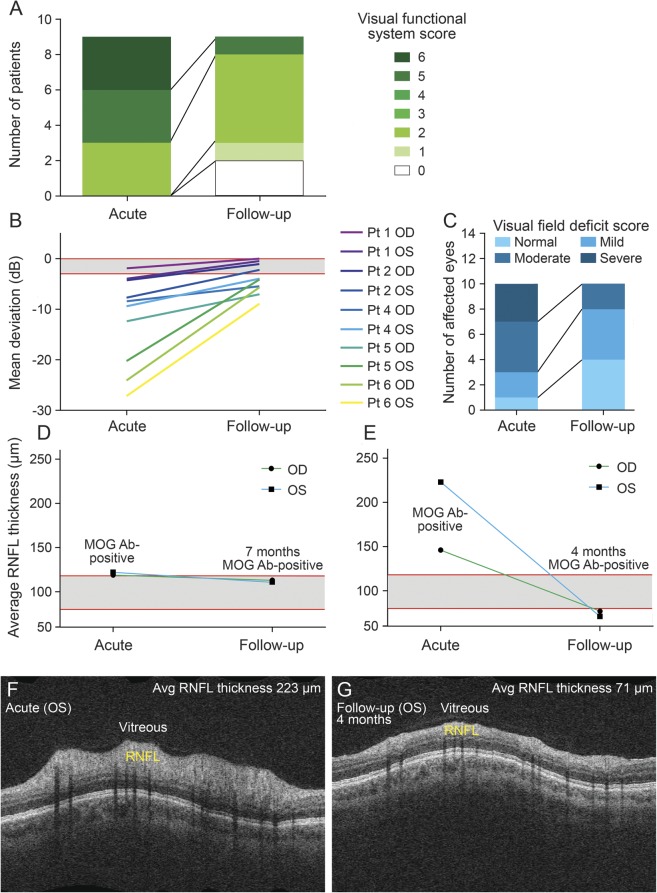
Results: MOG antibodies were detected in 9/23 AQP4 antibody-negative patients with NMO/NMOSD, compared to 1/76 patients with MS and 0/52 controls (p < 0.001). MOG antibodies were detected in 8/11 patients with BON, 0/10 patients with LETM, and 1/2 patients with sequential BON and LETM. Six of 9 MOG antibody-positive patients had a relapsing course. MOG antibody-positive patients had prominent optic disc swelling and were more likely to have a rapid response to steroid therapy and relapse on steroid cessation than MOG antibody-negative patients (p = 0.034 and p = 0.029, respectively). While 8/9 MOG antibody-positive patients had good follow-up visual acuity, one experienced sustained visual impairment, 3 had retinal nerve fiber layer thinning, and one had residual spinal disability.
Conclusions: MOG antibodies have a strong association with BON and may be a useful clinical biomarker. MOG antibody-associated BON is a relapsing disorder that is frequently steroid responsive and often steroid dependent. Failure to recognize the disorder early and institute immunotherapy promptly may be associated with sustained impairment.
Classification of evidence: This study provides Class II evidence that MOG antibodies are associated with AQP4 antibody-negative BON (sensitivity 69%, 95% confidence interval [CI] 42%-87%; specificity 99%, 95% CI 93.7%-99.8%).
Figures
Similar articles
-
MOG-IgG in NMO and related disorders: a multicenter study of 50 patients. Part 1: Frequency, syndrome specificity, influence of disease activity, long-term course, association with AQP4-IgG, and origin.J Neuroinflammation. 2016 Sep 26;13(1):279. doi: 10.1186/s12974-016-0717-1. J Neuroinflammation. 2016. PMID: 27788675 Free PMC article.
-
Neuromyelitis optica spectrum disorders with antibodies to myelin oligodendrocyte glycoprotein or aquaporin-4: Clinical and paraclinical characteristics in Algerian patients.J Neurol Sci. 2017 Oct 15;381:240-244. doi: 10.1016/j.jns.2017.08.3254. Epub 2017 Aug 31. J Neurol Sci. 2017. PMID: 28991690
-
Antibodies to MOG and AQP4 in children with neuromyelitis optica and limited forms of the disease.J Neurol Neurosurg Psychiatry. 2016 Aug;87(8):897-905. doi: 10.1136/jnnp-2015-311743. Epub 2015 Dec 8. J Neurol Neurosurg Psychiatry. 2016. PMID: 26645082
-
Neuromyelitis optica spectrum disorder: Pathogenesis, treatment, and experimental models.Mult Scler Relat Disord. 2019 Jan;27:412-418. doi: 10.1016/j.msard.2018.12.002. Epub 2018 Dec 3. Mult Scler Relat Disord. 2019. PMID: 30530071 Review.
-
Myelin oligodendrocyte glycoprotein antibodies in neuromyelitis optica spectrum disorder.Curr Opin Neurol. 2019 Feb;32(1):111-114. doi: 10.1097/WCO.0000000000000650. Curr Opin Neurol. 2019. PMID: 30562266 Review.
Cited by
-
MOG-IgG in NMO and related disorders: a multicenter study of 50 patients. Part 1: Frequency, syndrome specificity, influence of disease activity, long-term course, association with AQP4-IgG, and origin.J Neuroinflammation. 2016 Sep 26;13(1):279. doi: 10.1186/s12974-016-0717-1. J Neuroinflammation. 2016. PMID: 27788675 Free PMC article.
-
Anti-MOG antibodies are frequently associated with steroid-sensitive recurrent optic neuritis.Neurol Neuroimmunol Neuroinflamm. 2015 Jul 2;2(4):e131. doi: 10.1212/NXI.0000000000000131. eCollection 2015 Aug. Neurol Neuroimmunol Neuroinflamm. 2015. PMID: 26185777 Free PMC article. No abstract available.
-
Myelin oligodendrocyte glycoprotein-positive optic neuritis masquerading as pseudotumor cerebri at presentation.J Neurol. 2018 Sep;265(9):1985-1988. doi: 10.1007/s00415-018-8956-y. Epub 2018 Jun 25. J Neurol. 2018. PMID: 29938337
-
Structural and Functional Alterations in Visual Pathway After Optic Neuritis in MOG Antibody Disease: A Comparative Study With AQP4 Seropositive NMOSD.Front Neurol. 2021 Jun 9;12:673472. doi: 10.3389/fneur.2021.673472. eCollection 2021. Front Neurol. 2021. PMID: 34177778 Free PMC article.
-
Clinical course, therapeutic responses and outcomes in relapsing MOG antibody-associated demyelination.J Neurol Neurosurg Psychiatry. 2018 Feb;89(2):127-137. doi: 10.1136/jnnp-2017-316880. Epub 2017 Nov 15. J Neurol Neurosurg Psychiatry. 2018. PMID: 29142145 Free PMC article.
References
-
- Lennon VA, Wingerchuk DM, Kryzer TJ, et al. . A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet 2004;364:2106–2112 - PubMed
-
- Kitley J, Leite MI, Nakashima I, et al. . Prognostic factors and disease course in aquaporin-4 antibody-positive patients with neuromyelitis optica spectrum disorder from the United Kingdom and Japan. Brain 2012;135:1834–1849 - PubMed
-
- Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006;66:1485–1489 - PubMed
-
- Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica. Lancet Neurol 2007;6:805–815 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials