

Severity of retinopathy parallels the degree of parasite sequestration in the eyes and brains of malawian children with fatal cerebral malaria
- PMID: 25351204
- PMCID: PMC4442623
- DOI: 10.1093/infdis/jiu592
Severity of retinopathy parallels the degree of parasite sequestration in the eyes and brains of malawian children with fatal cerebral malaria
Abstract
Background: Malarial retinopathy (MR) has diagnostic and prognostic value in children with Plasmodium falciparum cerebral malaria (CM). A clinicopathological correlation between observed retinal changes during life and the degree of sequestration of parasitized red blood cells was investigated in ocular and cerebral vessels at autopsy.
Methods: In 18 Malawian children who died from clinically defined CM, we studied the intensity of sequestration and the maturity of sequestered parasites in the retina, in nonretinal ocular tissues, and in the brain.
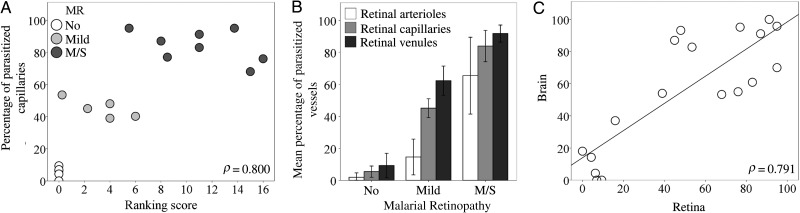
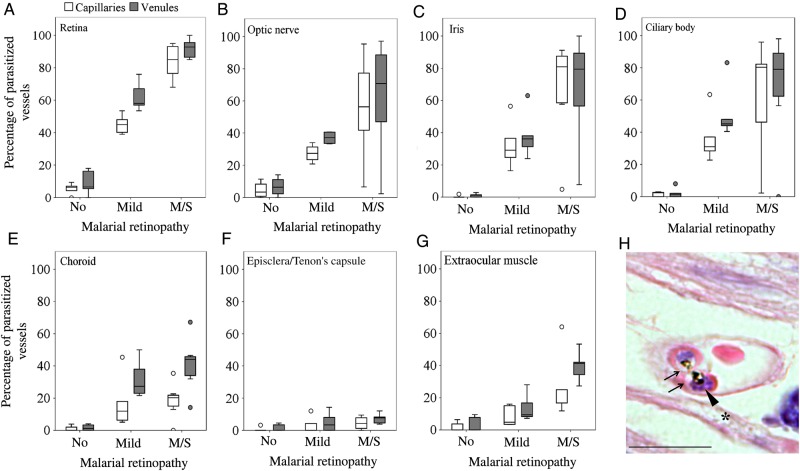
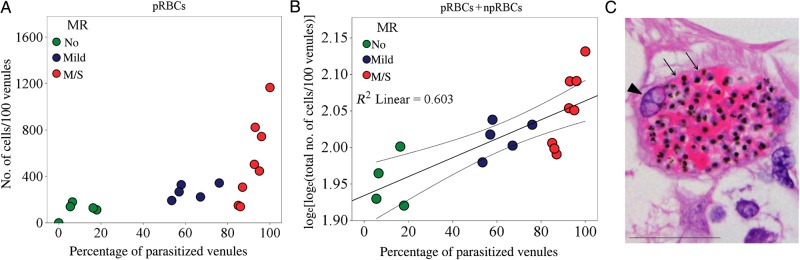
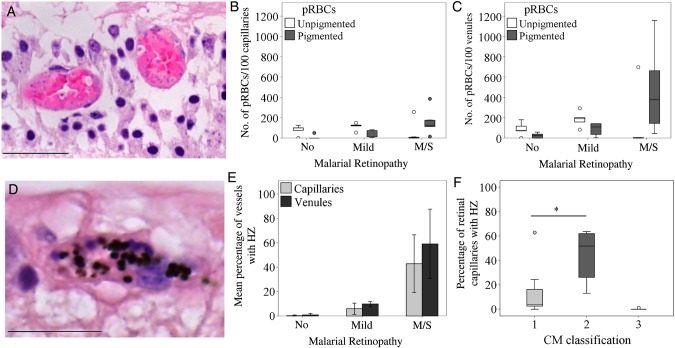
Results: Five children with clinically defined CM during life had other causes of death identified at autopsy, no MR, and scanty intracerebral sequestration. Thirteen children had MR and died from CM. MR severity correlated with percentage of microvessels parasitized in the retina, brain, and nonretinal tissues with some neuroectodermal components (all P < .01). In moderate/severe MR cases (n = 8), vascular congestion was more intense (ρ = 0.841; P < .001), sequestered parasites were more mature, and the quantity of extraerythrocytic hemozoin was higher, compared with mild MR cases (n = 5).
Conclusions: These data provide a histopathological basis for the known correlation between degrees of retinopathy and cerebral dysfunction in CM. In addition to being a valuable tool for clinical diagnosis, retinal observations give important information about neurovascular pathophysiology in pediatric CM.
Keywords: Plasmodium falciparum malaria; cerebral malaria; clinicopathological correlation; histopathology; malarial retinopathy; microvascular congestion; neurovasculature; parasite sequestration; pediatric coma; vascular pathology.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Figures
Similar articles
-
Retinal pathology of pediatric cerebral malaria in Malawi.PLoS One. 2009;4(1):e4317. doi: 10.1371/journal.pone.0004317. Epub 2009 Jan 29. PLoS One. 2009. PMID: 19177166 Free PMC article.
-
Sequestration and microvascular congestion are associated with coma in human cerebral malaria.J Infect Dis. 2012 Feb 15;205(4):663-71. doi: 10.1093/infdis/jir812. Epub 2011 Dec 29. J Infect Dis. 2012. PMID: 22207648 Free PMC article.
-
A histological method for quantifying Plasmodium falciparum in the brain in fatal paediatric cerebral malaria.Malar J. 2013 Jun 7;12:191. doi: 10.1186/1475-2875-12-191. Malar J. 2013. PMID: 23758807 Free PMC article.
-
Redefining cerebral malaria by including malaria retinopathy.Future Microbiol. 2011 Mar;6(3):349-55. doi: 10.2217/fmb.11.3. Future Microbiol. 2011. PMID: 21449844 Free PMC article. Review.
-
Cerebral malaria in children: using the retina to study the brain.Brain. 2014 Aug;137(Pt 8):2119-42. doi: 10.1093/brain/awu001. Epub 2014 Feb 26. Brain. 2014. PMID: 24578549 Free PMC article. Review.
Cited by
-
Pathophysiology and neurologic sequelae of cerebral malaria.Malar J. 2020 Jul 23;19(1):266. doi: 10.1186/s12936-020-03336-z. Malar J. 2020. PMID: 32703204 Free PMC article. Review.
-
Ocular Pathology of Cerebral Malaria.Methods Mol Biol. 2022;2470:749-763. doi: 10.1007/978-1-0716-2189-9_55. Methods Mol Biol. 2022. PMID: 35881387
-
A retinal model of cerebral malaria.Sci Rep. 2019 Mar 5;9(1):3470. doi: 10.1038/s41598-019-39143-z. Sci Rep. 2019. PMID: 30837488 Free PMC article.
-
Ocular Parasitosis Caused by Protozoan Infection during Travel: Focus on Prevention and Treatment.Int J Prev Med. 2018 Sep 17;9:79. doi: 10.4103/ijpvm.IJPVM_161_18. eCollection 2018. Int J Prev Med. 2018. PMID: 30283611 Free PMC article. Review.
-
Type I Interferon Receptor Variants in Gene Regulatory Regions are Associated with Susceptibility to Cerebral Malaria in Malawi.Am J Trop Med Hyg. 2018 Jun;98(6):1692-1698. doi: 10.4269/ajtmh.17-0887. Epub 2018 Apr 5. Am J Trop Med Hyg. 2018. PMID: 29637882 Free PMC article.
References
-
- Newton CR, Taylor TE, Whitten RO. Pathophysiology of fatal falciparum malaria in African children. Am J Trop Med Hyg 1998; 58:673–83. - PubMed
-
- Taylor TE, Fu WJ, Carr RA, et al. Differentiating the pathologies of cerebral malaria by postmortem parasite counts. Nat Med 2004; 10:143–5. - PubMed
-
- Hero M, Harding SP, Riva CE, Winstanley PA, Peshu N, Marsh K. Photographic and angiographic characterization of the retina of Kenyan children with severe malaria. Arch Ophthalmol 1997; 115:997–1003. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
