

IP-10 and MIG are compartmentalized at the site of disease during pleural and meningeal tuberculosis and are decreased after antituberculosis treatment
- PMID: 25274803
- PMCID: PMC4248780
- DOI: 10.1128/CVI.00499-14
IP-10 and MIG are compartmentalized at the site of disease during pleural and meningeal tuberculosis and are decreased after antituberculosis treatment
Abstract
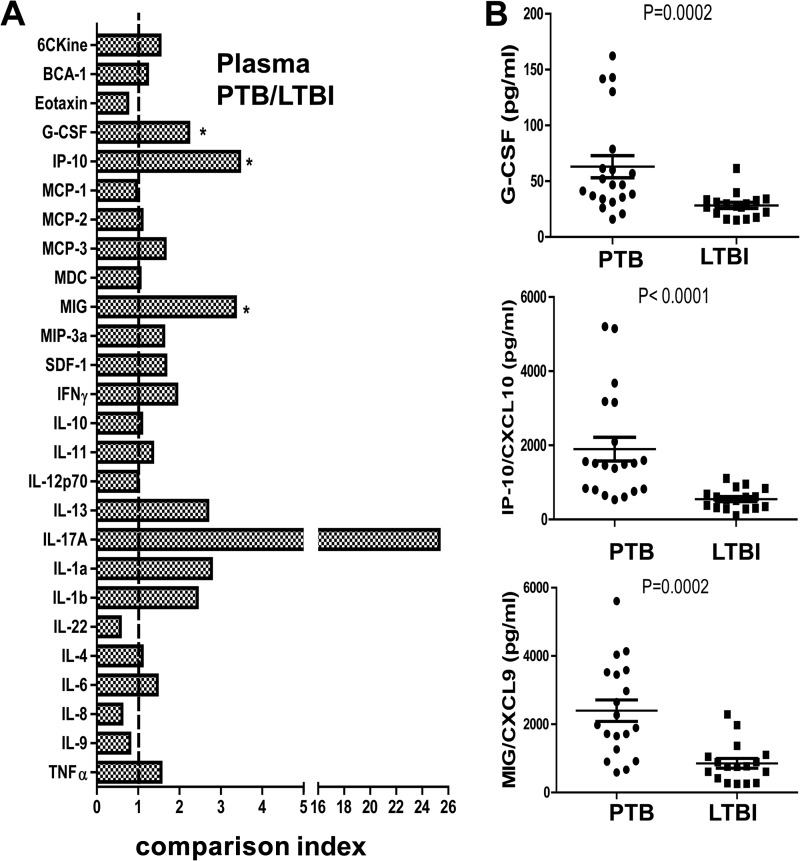
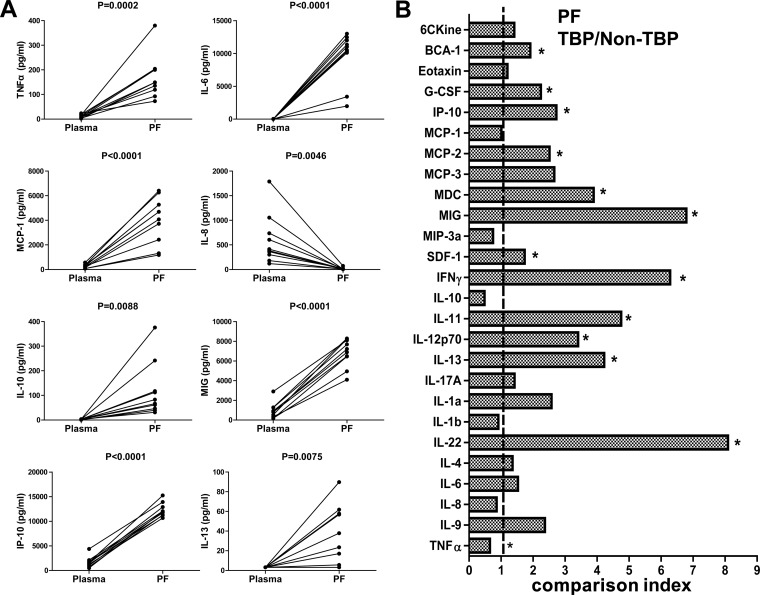
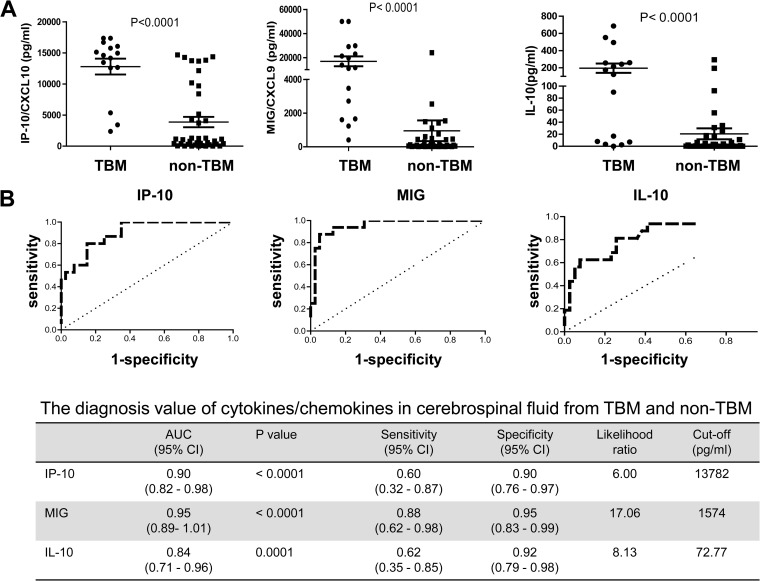
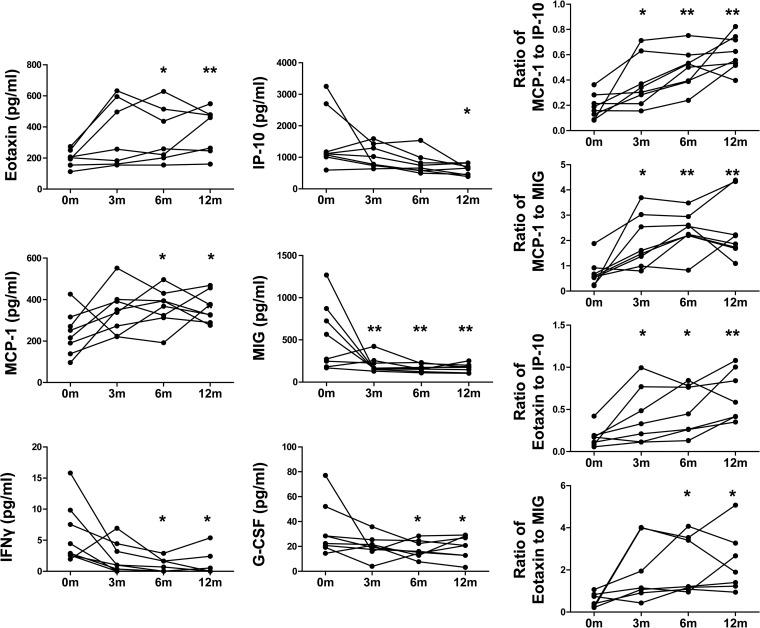
The diagnosis of active tuberculosis (TB) disease remains a challenge, especially in high-burden settings. Cytokines and chemokines are important in the pathogenesis of TB. Here we investigate the usefulness of circulating and compartmentalized cytokines/chemokines for diagnosis of TB. The levels of multiple cytokines/chemokines in plasma, pleural fluid (PF), and cerebrospinal fluid (CSF) were determined by Luminex liquid array-based multiplexed immunoassays. Three of 26 cytokines/chemokines in plasma were significantly different between TB and latent tuberculosis infection (LTBI). Among them, IP-10 and MIG had the highest diagnostic values, with an area under the receiver operating characteristic curve (ROC AUC) of 0.92 for IP-10 and 0.86 for MIG for distinguishing TB from LTBI. However, IP-10 and MIG levels in plasma were not different between TB and non-TB lung disease. In contrast, compartmentalized IP-10 and MIG in the PF and CSF showed promising diagnostic values in discriminating TB and non-TB pleural effusion (AUC = 0.87 for IP-10 and 0.93 for MIG), as well as TB meningitis and non-TB meningitis (AUC = 0.9 for IP-10 and 0.95 for MIG). A longitudinal study showed that the plasma levels of IP-10, MIG, granulocyte colony-stimulating factor (G-CSF), and gamma interferon (IFN-γ) decreased, while the levels of MCP-1/CCL2 and eotaxin-1/CCL11 increased, after successful treatment of TB. Our findings provide a practical methodology for discriminating active TB from LTBI by sequential IFN-γ release assays (IGRAs) and plasma IP-10 testing, while increased IP-10 and MIG at the site of infection (PF or CSF) can be used as a marker for distinguishing pleural effusion and meningitis caused by TB from those of non-TB origins.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures
Similar articles
-
Multiplex analysis of plasma cytokines/chemokines showing different immune responses in active TB patients, latent TB infection and healthy participants.Tuberculosis (Edinb). 2017 Dec;107:88-94. doi: 10.1016/j.tube.2017.07.013. Epub 2017 Aug 3. Tuberculosis (Edinb). 2017. PMID: 29050777
-
Discrimination between active and latent tuberculosis based on ratio of antigen-specific to mitogen-induced IP-10 production.J Clin Microbiol. 2015 Feb;53(2):504-10. doi: 10.1128/JCM.02758-14. Epub 2014 Nov 26. J Clin Microbiol. 2015. PMID: 25428147 Free PMC article.
-
Plasma cytokines and chemokines differentiate between active disease and non-active tuberculosis infection.J Infect. 2013 Apr;66(4):357-65. doi: 10.1016/j.jinf.2012.11.005. Epub 2012 Nov 20. J Infect. 2013. PMID: 23178506
-
Mig chemokine in primary biliary cirrhosis.Clin Ter. 2019 May-Jun;170(3):e211-e215. doi: 10.7417/CT.2019.2135. Clin Ter. 2019. PMID: 31173052 Review.
-
The Th1 chemokine MIG in Graves' ophthalmopathy.Clin Ter. 2019 Sep-Oct;170(5):e368-e372. doi: 10.7417/CT.2019.2162. Clin Ter. 2019. PMID: 31612195 Review.
Cited by
-
Advances in the diagnosis of tuberculous pleuritis.Ann Transl Med. 2016 Aug;4(15):282. doi: 10.21037/atm.2016.07.23. Ann Transl Med. 2016. PMID: 27570776 Free PMC article. Review.
-
Recent advances in understanding the human host immune response in tuberculous meningitis.Front Immunol. 2024 Jan 9;14:1326651. doi: 10.3389/fimmu.2023.1326651. eCollection 2023. Front Immunol. 2024. PMID: 38264653 Free PMC article. Review.
-
Cytokine and Chemokine mRNA Expressions after Mycobacterium tuberculosis-Specific Antigen Stimulation in Whole Blood from Hemodialysis Patients with Latent Tuberculosis Infection.Diagnostics (Basel). 2021 Mar 26;11(4):595. doi: 10.3390/diagnostics11040595. Diagnostics (Basel). 2021. PMID: 33810426 Free PMC article.
-
CXCL9/CXCL10 as biomarkers the monitoring of treatment responses in Pulmonary TB patients: a systematic review and meta-analysis.BMC Infect Dis. 2024 Sep 27;24(1):1037. doi: 10.1186/s12879-024-09939-0. BMC Infect Dis. 2024. PMID: 39333908 Free PMC article.
-
Plasma Cytokine Predictors of Tuberculosis Recurrence in Antiretroviral-Treated Human Immunodeficiency Virus-infected Individuals from Durban, South Africa.Clin Infect Dis. 2017 Sep 1;65(5):819-826. doi: 10.1093/cid/cix357. Clin Infect Dis. 2017. PMID: 29017282 Free PMC article.
References
-
- Shenai S, Amisano D, Ronacher K, Kriel M, Banada PP, Song T, Lee M, Joh JS, Winter J, Thayer R, Via LE, Kim S, Barry CE, 3rd, Walzl G, Alland D. 2013. Exploring alternative biomaterials for diagnosis of pulmonary tuberculosis in HIV-negative patients by use of the GeneXpert MTB/RIF assay. J. Clin. Microbiol. 51:4161–4166. 10.1128/JCM.01743-13. - DOI - PMC - PubMed
-
- Kim CH, Woo H, Hyun IG, Kim C, Choi JH, Jang SH, Park SM, Kim DG, Lee MG, Jung KS, Hyun J, Kim HS. 2014. A comparison between the efficiency of the Xpert MTB/RIF assay and nested PCR in identifying Mycobacterium tuberculosis during routine clinical practice. J. Thorac. Dis. 6:625–631. 10.3978/j.issn.2072-1439.2014.04.12. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
