

Body-mass index and risk of 22 specific cancers: a population-based cohort study of 5·24 million UK adults
- PMID: 25129328
- PMCID: PMC4151483
- DOI: 10.1016/S0140-6736(14)60892-8
Body-mass index and risk of 22 specific cancers: a population-based cohort study of 5·24 million UK adults
Abstract
Background: High body-mass index (BMI) predisposes to several site-specific cancers, but a large-scale systematic and detailed characterisation of patterns of risk across all common cancers adjusted for potential confounders has not previously been undertaken. We aimed to investigate the links between BMI and the most common site-specific cancers.
Methods: With primary care data from individuals in the Clinical Practice Research Datalink with BMI data, we fitted Cox models to investigate associations between BMI and 22 of the most common cancers, adjusting for potential confounders. We fitted linear then non-linear (spline) models; investigated effect modification by sex, menopausal status, smoking, and age; and calculated population effects.
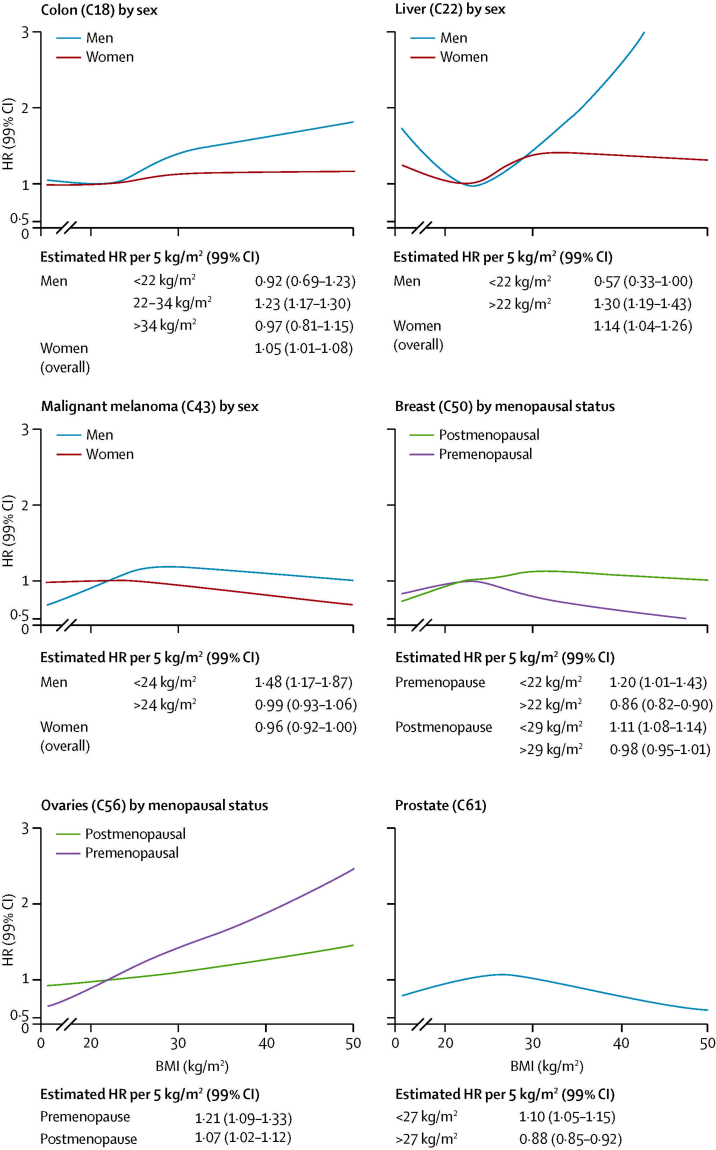
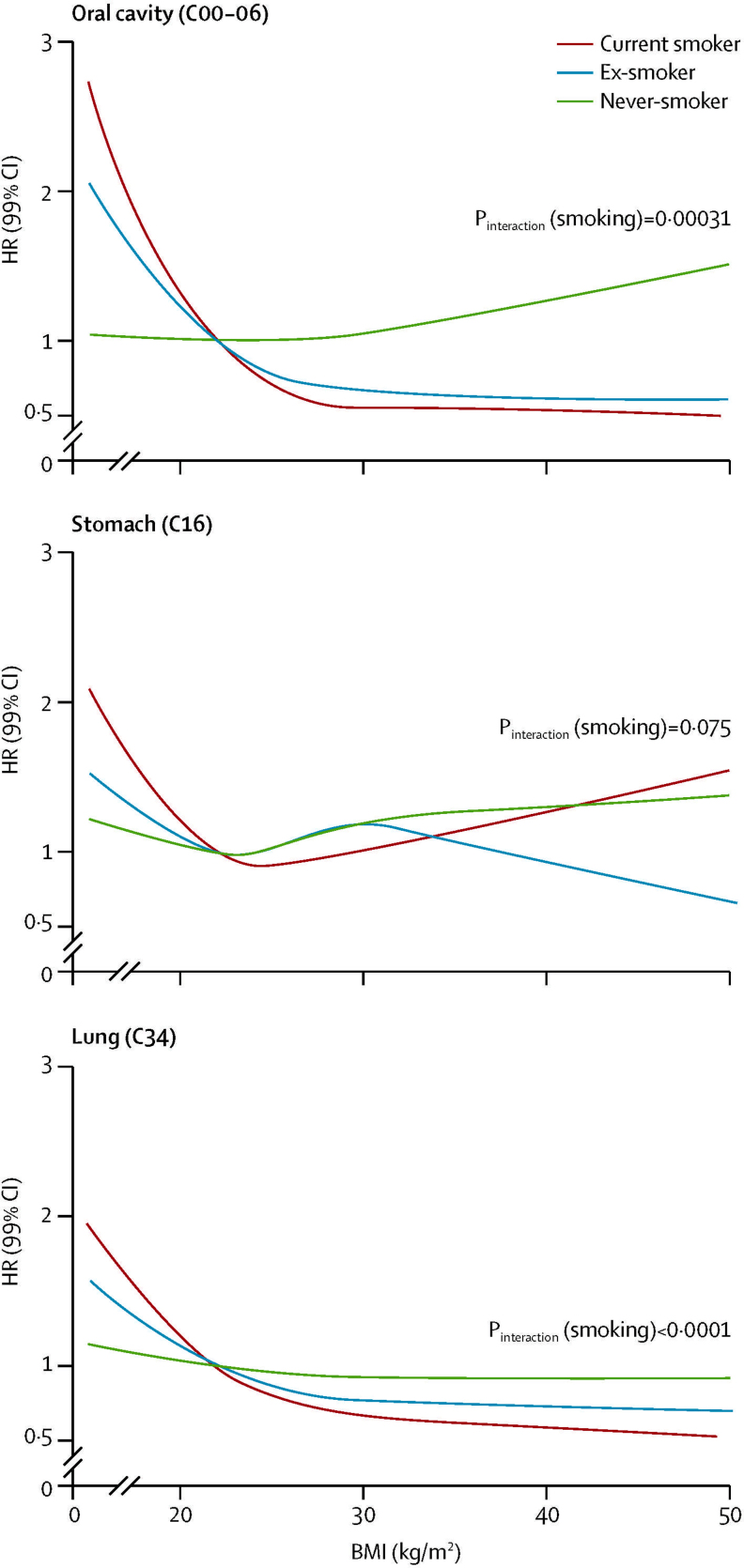
Findings: 5·24 million individuals were included; 166,955 developed cancers of interest. BMI was associated with 17 of 22 cancers, but effects varied substantially by site. Each 5 kg/m(2) increase in BMI was roughly linearly associated with cancers of the uterus (hazard ratio [HR] 1·62, 99% CI 1·56-1·69; p<0·0001), gallbladder (1·31, 1·12-1·52; p<0·0001), kidney (1·25, 1·17-1·33; p<0·0001), cervix (1·10, 1·03-1·17; p=0·00035), thyroid (1·09, 1·00-1·19; p=0·0088), and leukaemia (1·09, 1·05-1·13; p≤0·0001). BMI was positively associated with liver (1·19, 1·12-1·27), colon (1·10, 1·07-1·13), ovarian (1·09, 1.04-1.14), and postmenopausal breast cancers (1·05, 1·03-1·07) overall (all p<0·0001), but these effects varied by underlying BMI or individual-level characteristics. We estimated inverse associations with prostate and premenopausal breast cancer risk, both overall (prostate 0·98, 0·95-1·00; premenopausal breast cancer 0·89, 0·86-0·92) and in never-smokers (prostate 0·96, 0·93-0·99; premenopausal breast cancer 0·89, 0·85-0·94). By contrast, for lung and oral cavity cancer, we observed no association in never smokers (lung 0·99, 0·93-1·05; oral cavity 1·07, 0·91-1·26): inverse associations overall were driven by current smokers and ex-smokers, probably because of residual confounding by smoking amount. Assuming causality, 41% of uterine and 10% or more of gallbladder, kidney, liver, and colon cancers could be attributable to excess weight. We estimated that a 1 kg/m(2) population-wide increase in BMI would result in 3790 additional annual UK patients developing one of the ten cancers positively associated with BMI.
Interpretation: BMI is associated with cancer risk, with substantial population-level effects. The heterogeneity in the effects suggests that different mechanisms are associated with different cancer sites and different patient subgroups.
Funding: National Institute for Health Research, Wellcome Trust, and Medical Research Council.
Copyright © 2014 Bhaskaran et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd. All rights reserved.
Figures



Comment in
-
Overweight and obesity are linked to 10 common cancers and more than 12,000 UK cases.BMJ. 2014 Aug 14;349:g5183. doi: 10.1136/bmj.g5183. BMJ. 2014. PMID: 25128484 No abstract available.
-
Obesity: a certain and avoidable cause of cancer.Lancet. 2014 Aug 30;384(9945):727-8. doi: 10.1016/S0140-6736(14)61172-7. Epub 2014 Aug 13. Lancet. 2014. PMID: 25129326 No abstract available.
-
The obesity and cancer link.Ann Oncol. 2015 Feb;26(2):440-1. doi: 10.1093/annonc/mdu545. Epub 2014 Nov 18. Ann Oncol. 2015. PMID: 25411414 No abstract available.
-
[Fat people have common cancers].MMW Fortschr Med. 2014 Nov 13;156 Spec no 2:31. doi: 10.1007/s15006-014-3684-4. MMW Fortschr Med. 2014. PMID: 25552010 German. No abstract available.
-
[Obesity and cancer].Soins. 2014 Nov;(790):10. Soins. 2014. PMID: 25619087 French. No abstract available.
Similar articles
-
Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3·6 million adults in the UK.Lancet Diabetes Endocrinol. 2018 Dec;6(12):944-953. doi: 10.1016/S2213-8587(18)30288-2. Epub 2018 Oct 30. Lancet Diabetes Endocrinol. 2018. PMID: 30389323 Free PMC article.
-
Body mass index and waist circumference in relation to the risk of 26 types of cancer: a prospective cohort study of 3.5 million adults in Spain.BMC Med. 2021 Jan 14;19(1):10. doi: 10.1186/s12916-020-01877-3. BMC Med. 2021. PMID: 33441148 Free PMC article.
-
[Body mass index and cancer incidence:a prospective cohort study in northern China].Zhonghua Liu Xing Bing Xue Za Zhi. 2014 Mar;35(3):231-6. Zhonghua Liu Xing Bing Xue Za Zhi. 2014. PMID: 24831616 Chinese.
-
Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies.Lancet. 2008 Feb 16;371(9612):569-78. doi: 10.1016/S0140-6736(08)60269-X. Lancet. 2008. PMID: 18280327 Review.
-
Ovarian cancer and smoking: individual participant meta-analysis including 28,114 women with ovarian cancer from 51 epidemiological studies.Lancet Oncol. 2012 Sep;13(9):946-56. doi: 10.1016/S1470-2045(12)70322-4. Epub 2012 Aug 3. Lancet Oncol. 2012. PMID: 22863523 Free PMC article. Review.
Cited by
-
Hepatocellular carcinoma (HCC) in patients with Non-Alcoholic Fatty Liver Disease (NAFLD): screening, treatment and survival analysis in a Brazilian series.Clinics (Sao Paulo). 2022 Sep 7;77:100097. doi: 10.1016/j.clinsp.2022.100097. eCollection 2022. Clinics (Sao Paulo). 2022. PMID: 36088887 Free PMC article.
-
Adult obesity complications: challenges and clinical impact.Ther Adv Endocrinol Metab. 2020 Jun 22;11:2042018820934955. doi: 10.1177/2042018820934955. eCollection 2020. Ther Adv Endocrinol Metab. 2020. PMID: 32612803 Free PMC article. Review.
-
Effect of comedication of bupropion and other antidepressants on body mass index.Ther Adv Psychopharmacol. 2015 Jun;5(3):158-65. doi: 10.1177/2045125315577057. Ther Adv Psychopharmacol. 2015. PMID: 26199718 Free PMC article.
-
Associations of hypertension, diabetes and heart disease risk with body mass index in older Chinese adults: a population-based cohort study.BMJ Open. 2024 Jul 9;14(7):e083443. doi: 10.1136/bmjopen-2023-083443. BMJ Open. 2024. PMID: 38986550 Free PMC article.
-
A Mendelian randomization study identified obesity as a causal risk factor of uterine endometrial cancer in Japanese.Cancer Sci. 2020 Dec;111(12):4646-4651. doi: 10.1111/cas.14667. Epub 2020 Oct 27. Cancer Sci. 2020. PMID: 32981178 Free PMC article.
References
-
- WHO. World Health Statistics 2011. Geneva: World Health Organization.
-
- Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003;348:1625–1638. - PubMed
-
- Engeland A, Tretli S, Bjorge T. Height, body mass index, and ovarian cancer: a follow-up of 1·1 million Norwegian women. J Natl Cancer Inst. 2003;95:1244–1248. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
