

Acute chagas disease: new global challenges for an old neglected disease
- PMID: 25077613
- PMCID: PMC4117453
- DOI: 10.1371/journal.pntd.0003010
Acute chagas disease: new global challenges for an old neglected disease
Abstract
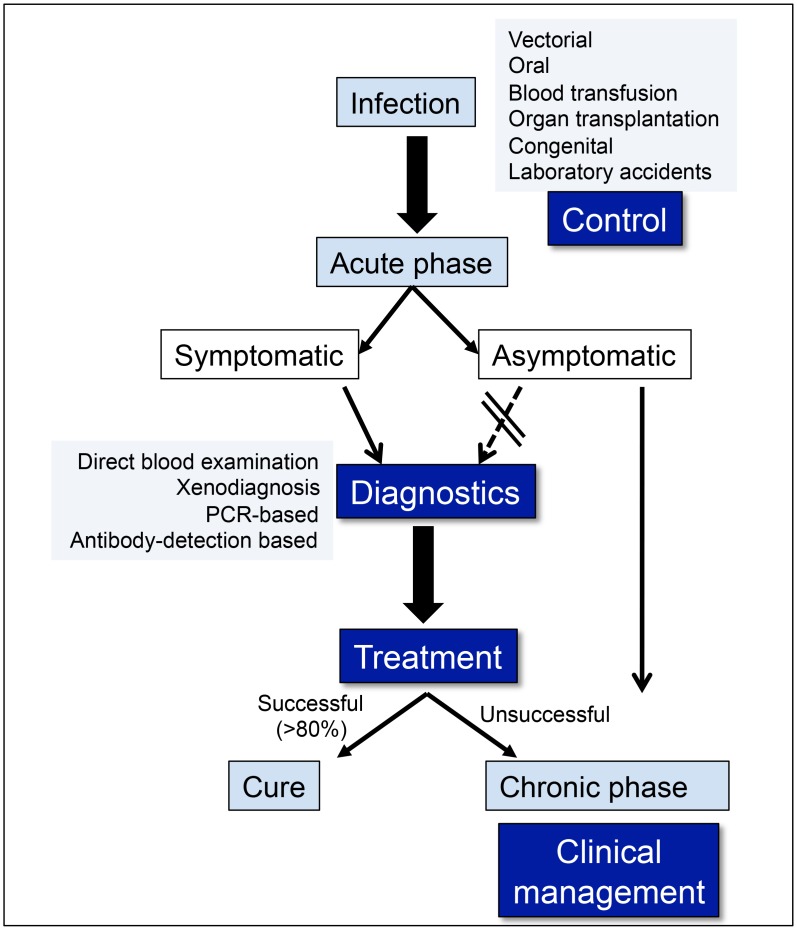
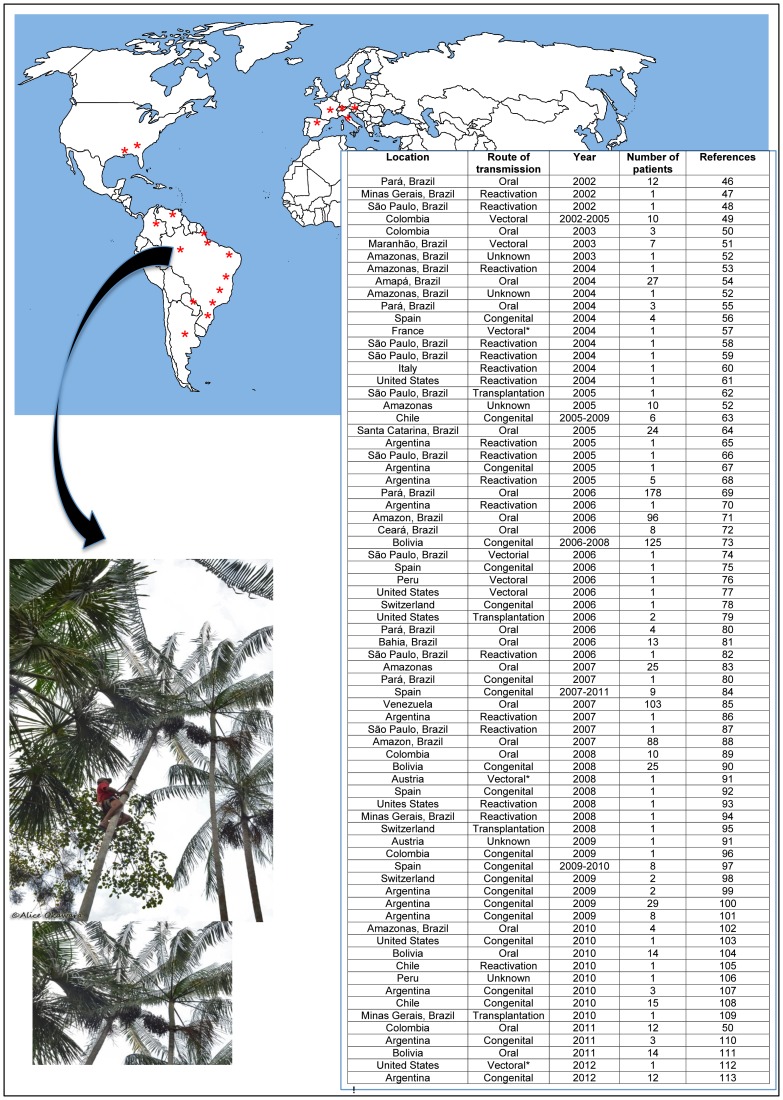
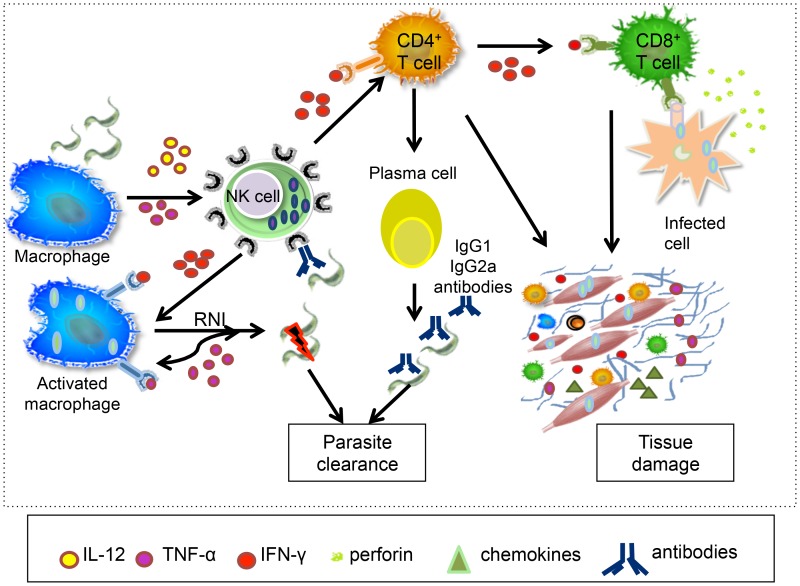
Chagas disease is caused by infection with the protozoan Trypanosoma cruzi, and although over 100 years have passed since the discovery of Chagas disease, it still presents an increasing problem for global public health. A plethora of information concerning the chronic phase of human Chagas disease, particularly the severe cardiac form, is available in the literature. However, information concerning events during the acute phase of the disease is scarce. In this review, we will discuss (1) the current status of acute Chagas disease cases globally, (2) the immunological findings related to the acute phase and their possible influence in disease outcome, and (3) reactivation of Chagas disease in immunocompromised individuals, a key point for transplantation and HIV infection management.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Old and new challenges in Chagas disease.Lancet Infect Dis. 2015 Nov;15(11):1347-56. doi: 10.1016/S1473-3099(15)00243-1. Epub 2015 Jul 28. Lancet Infect Dis. 2015. PMID: 26231478
-
Chagas disease in immunocompromised patients.Clin Microbiol Rev. 2024 Jun 13;37(2):e0009923. doi: 10.1128/cmr.00099-23. Epub 2024 Mar 28. Clin Microbiol Rev. 2024. PMID: 38546225 Review.
-
Acute Chagas disease in El Salvador 2000-2012 - need for surveillance and control.Mem Inst Oswaldo Cruz. 2014 Apr;109(2):256-8. doi: 10.1590/0074-0276140416. Epub 2014 Feb 17. Mem Inst Oswaldo Cruz. 2014. PMID: 24676660 Free PMC article.
-
Acute Chagas' disease: immunohistochemical characteristics of T cell infiltrate and its relationship with T. cruzi parasitic antigens.Acta Cardiol. 2005 Feb;60(1):33-7. doi: 10.2143/AC.60.1.2005046. Acta Cardiol. 2005. PMID: 15779849
-
Immunological control of Trypanosoma cruzi infection and pathogenesis of Chagas' disease.Int Arch Allergy Immunol. 1997 Oct;114(2):103-10. doi: 10.1159/000237653. Int Arch Allergy Immunol. 1997. PMID: 9338602 Review.
Cited by
-
The epidemiology of Chagas disease in the Americas.Lancet Reg Health Am. 2024 Sep 13;37:100881. doi: 10.1016/j.lana.2024.100881. eCollection 2024 Sep. Lancet Reg Health Am. 2024. PMID: 39474465 Free PMC article. Review.
-
Recombinant proteins as promising antigens applied to the immunodiagnosis of Chagas disease: a scoping review.Front Microbiol. 2024 Jul 30;15:1420226. doi: 10.3389/fmicb.2024.1420226. eCollection 2024. Front Microbiol. 2024. PMID: 39139374 Free PMC article.
-
Trypanosoma cruzi Phosphomannomutase and Guanosine Diphosphate-Mannose Pyrophosphorylase Ligandability Assessment.Antimicrob Agents Chemother. 2019 Sep 23;63(10):e01082-19. doi: 10.1128/AAC.01082-19. Print 2019 Oct. Antimicrob Agents Chemother. 2019. PMID: 31405854 Free PMC article.
-
Advances in nanocarriers as drug delivery systems in Chagas disease.Int J Nanomedicine. 2019 Aug 9;14:6407-6424. doi: 10.2147/IJN.S206109. eCollection 2019. Int J Nanomedicine. 2019. PMID: 31496694 Free PMC article. Review.
-
Metabolic syndrome agravates cardiovascular, oxidative and inflammatory dysfunction during the acute phase of Trypanosoma cruzi infection in mice.Sci Rep. 2019 Dec 11;9(1):18885. doi: 10.1038/s41598-019-55363-9. Sci Rep. 2019. PMID: 31827186 Free PMC article.
References
-
- World Health Organization (2013) Tropical Disease Research. Program for research and training tropical disease (TDR). Fact sheet N°340. Updated March 2013. Geneva: World Health Organization.
-
- Dias JCP (2007) Southern Cone Initiative for the elimination of domestic populations of Triatoma infestans and the interruption of transfusion Chagas disease. Historical aspects, present situation, and perspectives. Mem Inst Oswaldo Cruz 102: 11–18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
