

Low carbohydrate versus isoenergetic balanced diets for reducing weight and cardiovascular risk: a systematic review and meta-analysis
- PMID: 25007189
- PMCID: PMC4090010
- DOI: 10.1371/journal.pone.0100652
Low carbohydrate versus isoenergetic balanced diets for reducing weight and cardiovascular risk: a systematic review and meta-analysis
Erratum in
-
Correction: Low Carbohydrate versus Isoenergetic Balanced Diets for Reducing Weight and Cardiovascular Risk: A Systematic Review and Meta-Analysis.PLoS One. 2018 Jul 2;13(7):e0200284. doi: 10.1371/journal.pone.0200284. eCollection 2018. PLoS One. 2018. PMID: 29966000 Free PMC article.
Abstract
Background: Some popular weight loss diets restricting carbohydrates (CHO) claim to be more effective, and have additional health benefits in preventing cardiovascular disease compared to balanced weight loss diets.
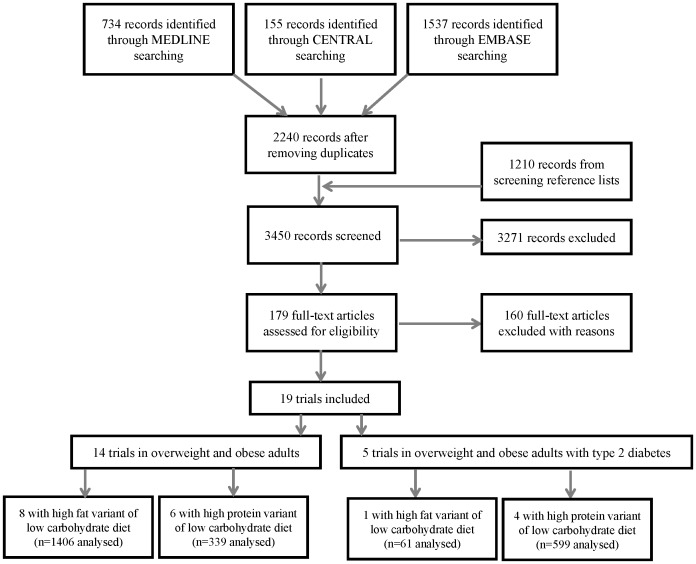
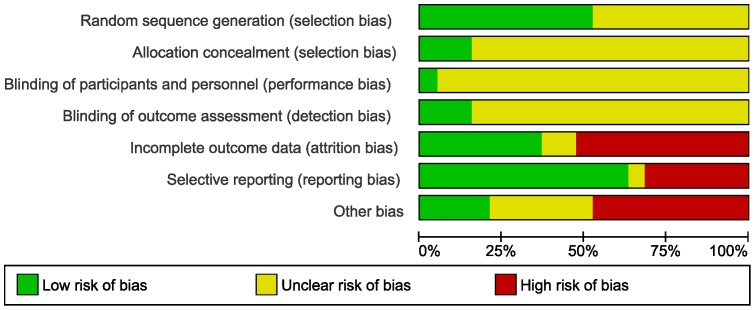
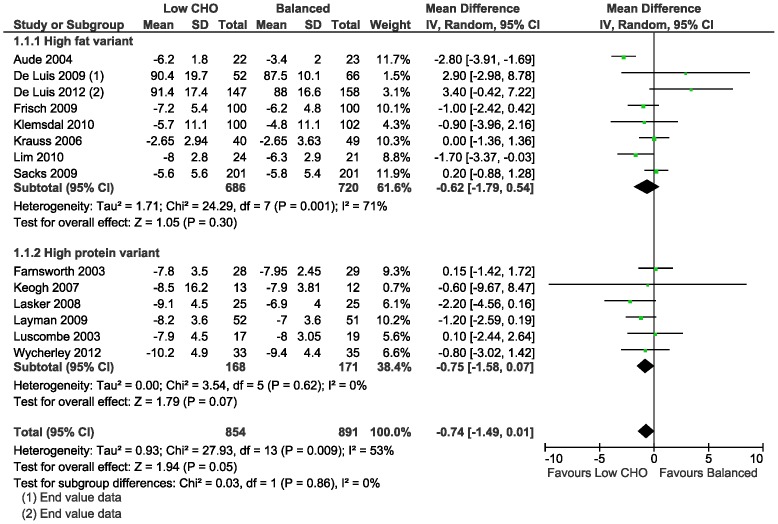
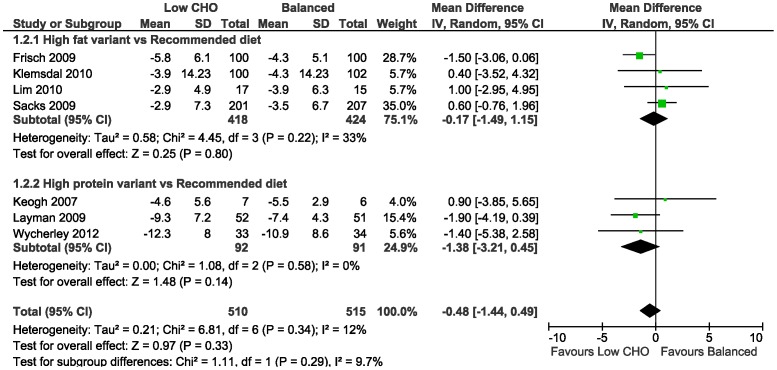
Methods and findings: We compared the effects of low CHO and isoenergetic balanced weight loss diets in overweight and obese adults assessed in randomised controlled trials (minimum follow-up of 12 weeks), and summarised the effects on weight, as well as cardiovascular and diabetes risk. Dietary criteria were derived from existing macronutrient recommendations. We searched Medline, EMBASE and CENTRAL (19 March 2014). Analysis was stratified by outcomes at 3-6 months and 1-2 years, and participants with diabetes were analysed separately. We evaluated dietary adherence and used GRADE to assess the quality of evidence. We calculated mean differences (MD) and performed random-effects meta-analysis. Nineteen trials were included (n = 3209); 3 had adequate allocation concealment. In non-diabetic participants, our analysis showed little or no difference in mean weight loss in the two groups at 3-6 months (MD 0.74 kg, 95%CI -1.49 to 0.01 kg; I2 = 53%; n = 1745, 14 trials; moderate quality evidence) and 1-2 years (MD 0.48 kg, 95%CI -1.44 kg to 0.49 kg; I2 = 12%; n = 1025; 7 trials, moderate quality evidence). Furthermore, little or no difference was detected at 3-6 months and 1-2 years for blood pressure, LDL, HDL and total cholesterol, triglycerides and fasting blood glucose (>914 participants). In diabetic participants, findings showed a similar pattern.
Conclusions: Trials show weight loss in the short-term irrespective of whether the diet is low CHO or balanced. There is probably little or no difference in weight loss and changes in cardiovascular risk factors up to two years of follow-up when overweight and obese adults, with or without type 2 diabetes, are randomised to low CHO diets and isoenergetic balanced weight loss diets.
Conflict of interest statement
Figures


Comment in
-
The universities of Stellenbosch/Cape Town low-carbohydrate diet review: Mistake or mischief?S Afr Med J. 2016 Dec 1;106(12):1179-1182. doi: 10.7196/SAMJ.2016.v106.i12.12072. S Afr Med J. 2016. PMID: 27917760
Similar articles
-
Low-carbohydrate versus balanced-carbohydrate diets for reducing weight and cardiovascular risk.Cochrane Database Syst Rev. 2022 Jan 28;1(1):CD013334. doi: 10.1002/14651858.CD013334.pub2. Cochrane Database Syst Rev. 2022. PMID: 35088407 Free PMC article. Review.
-
Comparison of dietary macronutrient patterns of 14 popular named dietary programmes for weight and cardiovascular risk factor reduction in adults: systematic review and network meta-analysis of randomised trials.BMJ. 2020 Apr 1;369:m696. doi: 10.1136/bmj.m696. BMJ. 2020. PMID: 32238384 Free PMC article.
-
Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: a meta-analysis of randomised controlled trials.Br J Nutr. 2016 Feb 14;115(3):466-79. doi: 10.1017/S0007114515004699. Br J Nutr. 2016. PMID: 26768850
-
Low protein diets for non-diabetic adults with chronic kidney disease.Cochrane Database Syst Rev. 2018 Oct 4;10(10):CD001892. doi: 10.1002/14651858.CD001892.pub4. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2020 Oct 29;10:CD001892. doi: 10.1002/14651858.CD001892.pub5 PMID: 30284724 Free PMC article. Updated.
-
Diets for weight management in adults with type 2 diabetes: an umbrella review of published meta-analyses and systematic review of trials of diets for diabetes remission.Diabetologia. 2022 Jan;65(1):14-36. doi: 10.1007/s00125-021-05577-2. Epub 2021 Nov 17. Diabetologia. 2022. PMID: 34796367 Free PMC article.
Cited by
-
A Modified Mediterranean Diet Improves Fasting and Postprandial Glucoregulation in Adults with Overweight and Obesity: A Pilot Study.Int J Environ Res Public Health. 2022 Nov 20;19(22):15347. doi: 10.3390/ijerph192215347. Int J Environ Res Public Health. 2022. PMID: 36430066 Free PMC article. Clinical Trial.
-
Application of n-of-1 Clinical Trials in Personalized Nutrition Research: A Trial Protocol for Westlake N-of-1 Trials for Macronutrient Intake (WE-MACNUTR).Curr Dev Nutr. 2020 Aug 26;4(9):nzaa143. doi: 10.1093/cdn/nzaa143. eCollection 2020 Sep. Curr Dev Nutr. 2020. PMID: 32968703 Free PMC article.
-
Effect of carbohydrate restriction on body weight in overweight and obese adults: a systematic review and dose-response meta-analysis of 110 randomized controlled trials.Front Nutr. 2023 Dec 6;10:1287987. doi: 10.3389/fnut.2023.1287987. eCollection 2023. Front Nutr. 2023. PMID: 38125726 Free PMC article.
-
Optimal Dietary Strategies for Prevention of Atherosclerotic Cardiovascular Disease in Diabetes: Evidence and Recommendations.Curr Cardiol Rep. 2019 Oct 17;21(11):132. doi: 10.1007/s11886-019-1232-7. Curr Cardiol Rep. 2019. PMID: 31624930 Review.
-
Small Dense Low-Density Lipoprotein Cholesterol Levels in Breakfast Skippers and Staple Foods Skippers.J Atheroscler Thromb. 2023 Oct 1;30(10):1376-1388. doi: 10.5551/jat.64024. Epub 2023 Mar 7. J Atheroscler Thromb. 2023. PMID: 36878535 Free PMC article.
References
-
- Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, et al. (2011) The global obesity pandemic: shaped by global drivers and local environments. Lancet 378: 804–814. - PubMed
-
- World Health Organization (2004) Global strategy on diet, physical activity and health. World Health Assembly Resolution 57.17. Geneva: World Health Organization
-
- World Health Organization (2010) Global status report on noncommunicable diseases 2010. Geneva: World Health Organization
-
- Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K (2007) The burden and costs of chronic diseases in low-income and middle-income countries. Lancet 370: 1929–1938. - PubMed
-
- World Health Organization (2008) The global burden of disease: 2004 update. Geneva, World Health Organization, 2008. Geneva: World Health Organization
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
