

Takayasu Arteritis in the pediatric population: a contemporary United States-based single center cohort
- PMID: 24955077
- PMCID: PMC4065084
- DOI: 10.1186/1546-0096-12-21
Takayasu Arteritis in the pediatric population: a contemporary United States-based single center cohort
Abstract
Background: Takayasu Arteritis is an idiopathic, chronic, large vessel vasculitis involving the aorta and its primary branches. Few studies have been done in pediatric patients to date with the largest case series of US patients published in 2003 consisting of only 6 patients.
Methods: A retrospective chart review was performed on all patients seen at Cleveland Clinic Children's up until 2012 who met EULAR/PRINTO/PRES classification criteria for childhood Takayasu Arteritis.
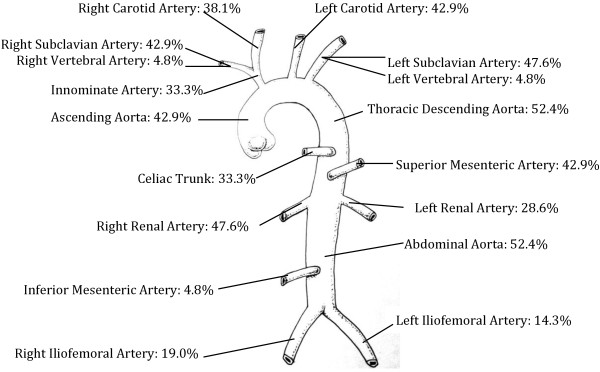
Results: Twenty-one patients with a mean follow up of 2.3 years were studied. Weight loss, fatigue, and anorexia were the most common presenting complaints. 57.1% of patients were hypertensive at first visit. The most common examintation finding was diminished pulses (61.9%), followed by bruits, and then murmurs. Thoracic aorta stenosis was the most common vascular abnormality. Seven of twenty-one patients responded well to methotrexate and prednisone alone. Ten of twenty-one patients required an additional medication for symptom and disease control (infliximab most commonly). About two-thirds of patients required at least one anti-hypertensive medication. Eight of the twenty-one patients required surgical intervention for severe disease refractory to medications (renal artery stenosis being the most common indication). Almost all patients reported symptomatic improvement after surgical intervention. Two of the eight patients required a second surgery for return of symptoms. Disease sequelae included arterial aneurysms, resolved heart failure, and hypertensive emergencies.
Conclusion: Our study emphasizes that constitutional symptoms coupled with objective findings of diminished pulses, bruits, and hypertension should raise clinical suspicion for Takayasu Arteritis in pediatric patients. Pharmacologic therapy alone can be successful in controlling disease progression, however surgery was successful in minimizing symptoms when medical therapies failed.
Keywords: Children; Cleveland Clinic Children’s Center for Pediatric Rheumatology; Takayasu Arteritis; United States; Vasculitis.
Figures
Similar articles
-
Early diagnosis of pediatric Takayasu arteritis (TA) not fullfiling the ACR criteria.Clin Exp Rheumatol. 2009 Jan-Feb;27(1 Suppl 52):S140. Clin Exp Rheumatol. 2009. PMID: 19646360 No abstract available.
-
Takayasu arteritis and large-vessel giant cell arteritis in Italian population. Comprehensive analysis from a single institutional cohort of 184 cases.Semin Arthritis Rheum. 2023 Apr;59:152173. doi: 10.1016/j.semarthrit.2023.152173. Epub 2023 Feb 8. Semin Arthritis Rheum. 2023. PMID: 36780709
-
Demographic, Clinical, and Radiologic Characteristics of a Cohort of Patients with Takayasu Arteritis.Am J Med. 2019 May;132(5):647-651. doi: 10.1016/j.amjmed.2018.12.017. Epub 2019 Jan 4. Am J Med. 2019. PMID: 30615861
-
Diagnostic and classification criteria of Takayasu arteritis.J Autoimmun. 2014 Feb-Mar;48-49:79-83. doi: 10.1016/j.jaut.2014.01.012. Epub 2014 Jan 21. J Autoimmun. 2014. PMID: 24461381 Review.
-
[Takayasu's arteritis--case report and review of the literature].Rev Med Suisse Romande. 2000 Oct;120(10):777-80. Rev Med Suisse Romande. 2000. PMID: 11109906 Review. French.
Cited by
-
Pediatric-onset Takayasu's arteritis: clinical features and short-term outcome.Rheumatol Int. 2015 Oct;35(10):1701-6. doi: 10.1007/s00296-015-3272-7. Epub 2015 Apr 24. Rheumatol Int. 2015. PMID: 25903354
-
Abdominal pain as the presenting symptom of Takayasu arteritis in an adolescent male: A case report.Medicine (Baltimore). 2018 Jun;97(26):e11326. doi: 10.1097/MD.0000000000011326. Medicine (Baltimore). 2018. PMID: 29953023 Free PMC article.
-
Incidental necrotizing aortitis in a child.Forensic Sci Med Pathol. 2017 Jun;13(2):252-254. doi: 10.1007/s12024-017-9842-0. Epub 2017 Mar 6. Forensic Sci Med Pathol. 2017. PMID: 28261753 No abstract available.
-
Non-specific aortoarteritis (NSAA) in children: a prospective observational study.BMJ Paediatr Open. 2021 Aug 9;5(1):e001106. doi: 10.1136/bmjpo-2021-001106. eCollection 2021. BMJ Paediatr Open. 2021. PMID: 34435143 Free PMC article.
-
Clinical course of 602 patients with Takayasu's arteritis: comparison between Childhood-onset versus adult onset disease.Rheumatology (Oxford). 2021 May 14;60(5):2246-2255. doi: 10.1093/rheumatology/keaa569. Rheumatology (Oxford). 2021. PMID: 33179052 Free PMC article.
References
-
- Jain S, Sharma N, Singh S, Bali HK, Kumar L, Sharma BK. Takayasu arteritis in children and young Indians. Int J Cardiol. 2000;75(Suppl 1):S153–S157. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
