

Autoantibodies to apolipoprotein A-1 as a biomarker of cardiovascular autoimmunity
- PMID: 24944761
- PMCID: PMC4062126
- DOI: 10.4330/wjc.v6.i5.314
Autoantibodies to apolipoprotein A-1 as a biomarker of cardiovascular autoimmunity
Abstract
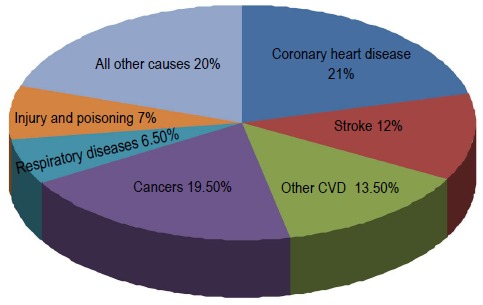
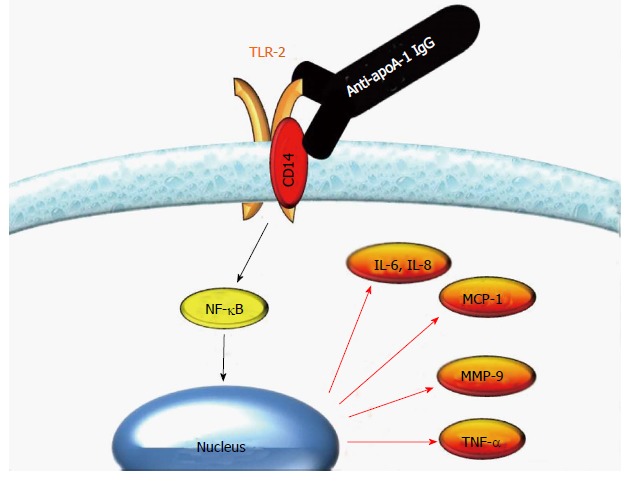
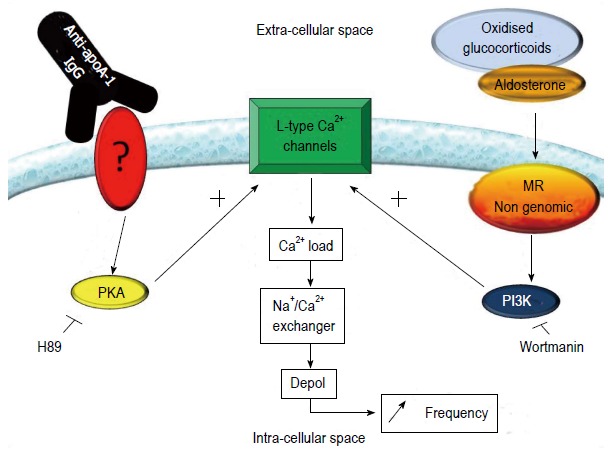
Immune-driven inflammation plays an important part in atherogenesis and is therefore believed to be key to the development of cardiovascular disease (CVD), which is currently the leading cause of death in the Western world. By fulfilling some of the Koch postulates, atherogenesis has even been proposed to be considered as an autoimmune disease, raising the hope that CVD could be prevented by immunomodulation. Nevertheless, the role of the immune system and autoimmune reactions in atherosclerosis appear to be a double edged-sword, with both pro-atherogenic and anti-atherogenic attributes. Hence, if immunomodulation is to become a therapeutic option for atherosclerosis and CVD, it will be crucial to correctly identify patients who might benefit from targeted suppression of deleterious autoimmune responses. This could be achieved, for example, by the detection of disease-associated autoantibodies. In this work, we will review the currently available clinical, in vitro, and animal studies dedicated to autoantibodies against apolipoprotein A-1 (anti-apoA-1 IgG), the major proteic fraction of high density lipoprotein. Current clinical studies indicate that high levels of anti-apoA-1 IgG are associated with a worse cardiovascular prognosis. In addition, in vitro and animal studies indicate a pro-inflammatory and pro-atherogenic role, supporting the hypothesis that these autoantibodies may play a direct causal role in CVD, and furthermore that they could potentially represent a therapeutic target for CVD in the future.
Keywords: Apolipoprotein A-1; Atherosclerosis; Autoantibodies; Autoimmunity; Biomarkers; Cardiovascular disease.
Figures
Similar articles
-
Autoantibodies to apolipoprotein A-1 in cardiovascular diseases: current perspectives.Clin Dev Immunol. 2012;2012:868251. doi: 10.1155/2012/868251. Epub 2012 Nov 20. Clin Dev Immunol. 2012. PMID: 23227091 Free PMC article. Review.
-
Anti-apolipoprotein A-1 autoantibodies as risk biomarker for cardiovascular diseases in type 2 diabetes mellitus.J Diabetes Complications. 2016 May-Jun;30(4):580-5. doi: 10.1016/j.jdiacomp.2016.02.014. Epub 2016 Feb 21. J Diabetes Complications. 2016. PMID: 26965796
-
Autoantibody to apolipoprotein A-1 in hepatitis C virus infection: a role in atherosclerosis?Hepatol Int. 2018 Jan;12(1):17-25. doi: 10.1007/s12072-018-9842-5. Epub 2018 Feb 8. Hepatol Int. 2018. PMID: 29423541 Free PMC article.
-
Humoral Immunity Against HDL Particle: A New Perspective in Cardiovascular Diseases?Curr Pharm Des. 2019;25(29):3128-3146. doi: 10.2174/1381612825666190830164917. Curr Pharm Des. 2019. PMID: 31470782 Review.
-
Association between anti-apolipoprotein A-1 antibodies and cardiovascular disease in the general population. Results from the CoLaus study.Thromb Haemost. 2016 Sep 27;116(4):764-71. doi: 10.1160/TH16-03-0248. Epub 2016 Jul 7. Thromb Haemost. 2016. PMID: 27384400
Cited by
-
ApoA1 and ApoA1-specific self-antibodies in cardiovascular disease.Lab Invest. 2016 Jul;96(7):708-18. doi: 10.1038/labinvest.2016.56. Epub 2016 May 16. Lab Invest. 2016. PMID: 27183204 Review.
-
Role of Clinical Characteristics and Biomarkers at Admission to Predict One-Year Mortality in Elderly Patients with Pneumonia.J Clin Med. 2021 Dec 25;11(1):105. doi: 10.3390/jcm11010105. J Clin Med. 2021. PMID: 35011845 Free PMC article.
-
A Master Autoantigen-ome Links Alternative Splicing, Female Predilection, and COVID-19 to Autoimmune Diseases.bioRxiv [Preprint]. 2021 Aug 4:2021.07.30.454526. doi: 10.1101/2021.07.30.454526. bioRxiv. 2021. Update in: J Transl Autoimmun. 2022;5:100147. doi: 10.1016/j.jtauto.2022.100147. PMID: 34373855 Free PMC article. Updated. Preprint.
-
Autoantibodies to Oxidatively Modified Peptide: Potential Clinical Application in Coronary Artery Disease.Diagnostics (Basel). 2022 Sep 20;12(10):2269. doi: 10.3390/diagnostics12102269. Diagnostics (Basel). 2022. PMID: 36291959 Free PMC article.
-
Low Level Antibodies Against Alpha-Tropomyosin Are Associated With Increased Risk of Coronary Heart Disease.Front Pharmacol. 2020 Feb 27;11:195. doi: 10.3389/fphar.2020.00195. eCollection 2020. Front Pharmacol. 2020. PMID: 32174839 Free PMC article.
References
-
- Eyre H, Kahn R, Robertson RM, Clark NG, Doyle C, Hong Y, Gansler T, Glynn T, Smith RA, Taubert K, et al. Preventing cancer, cardiovascular disease, and diabetes: a common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. Circulation. 2004;109:3244–3255. - PubMed
-
- Naghavi M, Falk E, Hecht HS, Jamieson MJ, Kaul S, Berman D, Fayad Z, Budoff MJ, Rumberger J, Naqvi TZ, et al. From vulnerable plaque to vulnerable patient--Part III: Executive summary of the Screening for Heart Attack Prevention and Education (SHAPE) Task Force report. Am J Cardiol. 2006;98:2H–15H. - PubMed
-
- Murphy TP, Dhangana R, Pencina MJ, Zafar AM, D’Agostino RB. Performance of current guidelines for coronary heart disease prevention: optimal use of the Framingham-based risk assessment. Atherosclerosis. 2011;216:452–457. - PubMed
-
- Nasir K, Michos ED, Blumenthal RS, Raggi P. Detection of high-risk young adults and women by coronary calcium and National Cholesterol Education Program Panel III guidelines. J Am Coll Cardiol. 2005;46:1931–1936. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
