

Intraoperative blood loss during surgical treatment of low-rectal cancer by abdominosacral resection is higher than during extra-levator abdominosacral amputation of the rectum
- PMID: 24904664
- PMCID: PMC4042050
- DOI: 10.5114/aoms.2014.42582
Intraoperative blood loss during surgical treatment of low-rectal cancer by abdominosacral resection is higher than during extra-levator abdominosacral amputation of the rectum
Abstract
Introduction: Abdominosacral resection (ASR) usually required blood transfusions, which are virtually no longer in use in the modified abdominosacral amputation of the rectum (ASAR). The aim of this study was to compare the intra-operative bleeding in low-rectal patients subjected to ASR or ASAR.
Material and methods: The study included low-rectal cancer patients subjected to ASR (n = 114) or ASAR (n = 46) who were retrospectively compared in terms of: 1) the frequency of blood transfusions during surgery and up to 24 h thereafter; 2) the volume of intraoperative blood loss (ml of blood transfused) during surgery and up to 24 h thereafter; 3) hemoglobin concentrations (Hb) 1, 3 and 5 days after surgery; 4) the duration of hospitalization.
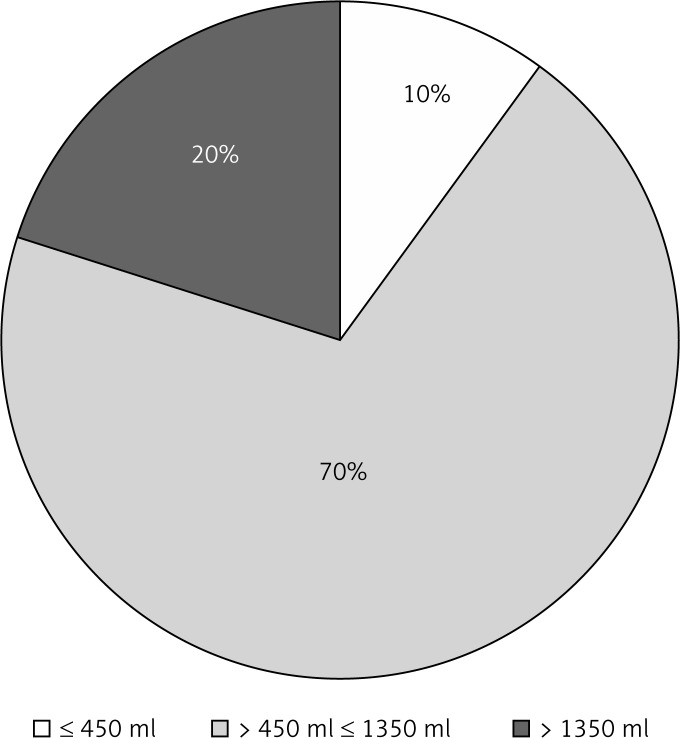
Results: Blood transfusions were necessary in 107 ASR patients but in none of those subjected to ASAR (p < 0.001). Median blood loss in the ASR group was 800 ml (range: 100-4500 ml). The differences between the groups in median Hb determined 1, 3 and 5 days following surgery were insignificant. The proportions of patients with abnormal values of Hb, however, were significantly higher in the ASR group on postoperative days 1 and 3 (day 1: 71.9% vs. 19.6% in the ASAR group, p = 0.025; day 3: 57.% vs. 13.0%, p = 0.009). Average postoperative hospitalization in ASR patients was 13 days compared to 9 days in the ASAR group (p = 0.031).
Conclusions: Abdominosacral amputation of the rectum predominates over ASR in terms of the prevention of intra- and postoperative bleeding due to the properly defined surgical plane in low-rectal cancer patients.
Keywords: abdominosacral amputation; blood loss; rectal cancer; total mesorectal excision.
Figures


Similar articles
-
[Comparison of clinical efficacy among different surgical methods for presacral recurrent rectal cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2020 May 25;23(5):466-471. doi: 10.3760/cma.j.cn.441530-20200210-00045. Zhonghua Wei Chang Wai Ke Za Zhi. 2020. PMID: 32842426 Chinese.
-
Therapeutic results in low-rectal cancer patients treated with abdominosacral resection are similar to those obtained by means of anterior resection in mid- and upper-rectal cancer cases.Eur J Surg Oncol. 2007 Apr;33(3):320-3. doi: 10.1016/j.ejso.2006.09.012. Epub 2006 Oct 13. Eur J Surg Oncol. 2007. PMID: 17046192
-
Abdominosacral amputation of the rectum for low rectal cancers: ten years of experience.Ann Surg Oncol. 2009 Aug;16(8):2211-7. doi: 10.1245/s10434-009-0517-2. Epub 2009 May 19. Ann Surg Oncol. 2009. PMID: 19452225
-
A comparison of published rates of resection margin involvement and intra-operative perforation between standard and 'cylindrical' abdominoperineal excision for low rectal cancer.Colorectal Dis. 2013 Jan;15(1):57-65. doi: 10.1111/j.1463-1318.2012.03167.x. Colorectal Dis. 2013. PMID: 22757637 Review.
-
Abdominosacral resection for midrectal cancer.Hepatogastroenterology. 1992 Jun;39(3):207-11. Hepatogastroenterology. 1992. PMID: 1505890 Review.
Cited by
-
MRI Evaluation of Extramural Venous Invasion (EMVI) with Rectal Carcinoma Using High Resolution T2 and Combination of High Resolution T2 and Contrast Enhanced T1 Weighted Imaging.Acta Inform Med. 2021 Jun;29(2):113-117. doi: 10.5455/aim.2021.29.113-117. Acta Inform Med. 2021. PMID: 34584334 Free PMC article.
References
-
- Nagtegaal ID, van de Velde CJH, Marijnen CAM, van Krieken JHJM, Quirke P. Low rectal cancer: a call for a change of approach in abdominoperineal resection. J Clin Oncol. 2005;23:9257–64. - PubMed
-
- Miles WE. A method of performing abdominoperineal excision for carcinoma of the rectum of the terminal portion of the pelvic colon. Lancet. 1908;2:1812–3. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources