

Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies
- PMID: 24690623
- PMCID: PMC3972416
- DOI: 10.1136/bmj.g1903
Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies
Abstract
Objective: To evaluate the extent to which circulating biomarker and supplements of vitamin D are associated with mortality from cardiovascular, cancer, or other conditions, under various circumstances.
Design: Systematic review and meta-analysis of observational studies and randomised controlled trials.
Data sources: Medline, Embase, Cochrane Library, and reference lists of relevant studies to August 2013; correspondance with investigators.
Study selection: Observational cohort studies and randomised controlled trials in adults, which reported associations between vitamin D (measured as circulating 25-hydroxyvitamin D concentration or vitamin D supplement given singly) and cause specific mortality outcomes.
Data extraction: Data were extracted by two independent investigators, and a consensus was reached with involvement of a third. Study specific relative risks from 73 cohort studies (849,412 participants) and 22 randomised controlled trials (vitamin D given alone versus placebo or no treatment; 30,716 participants) were meta-analysed using random effects models and were grouped by study and population characteristics.
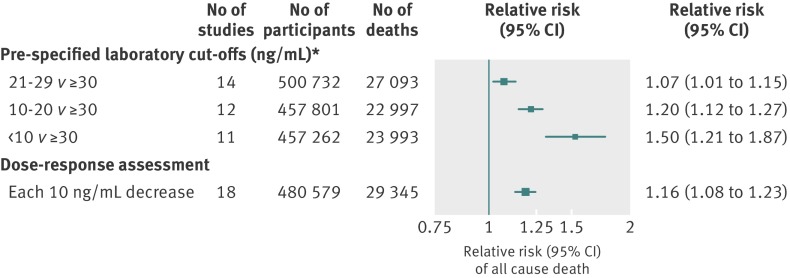
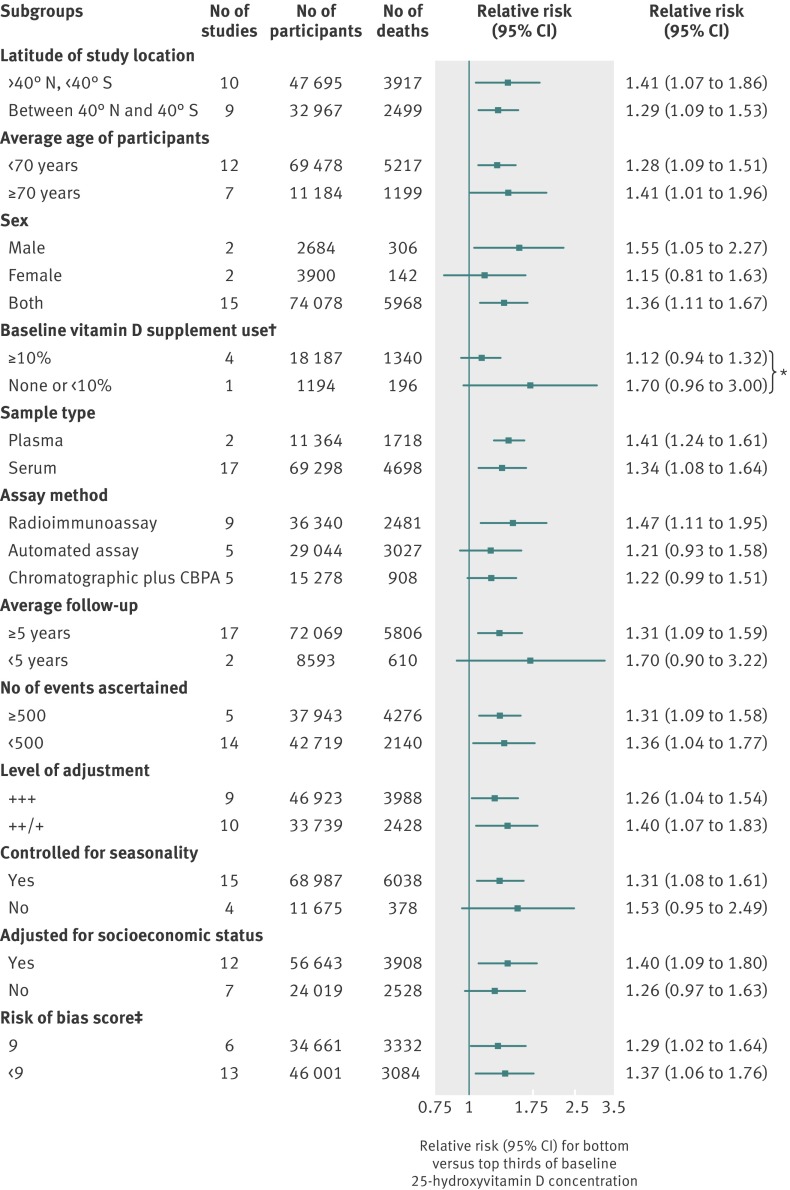
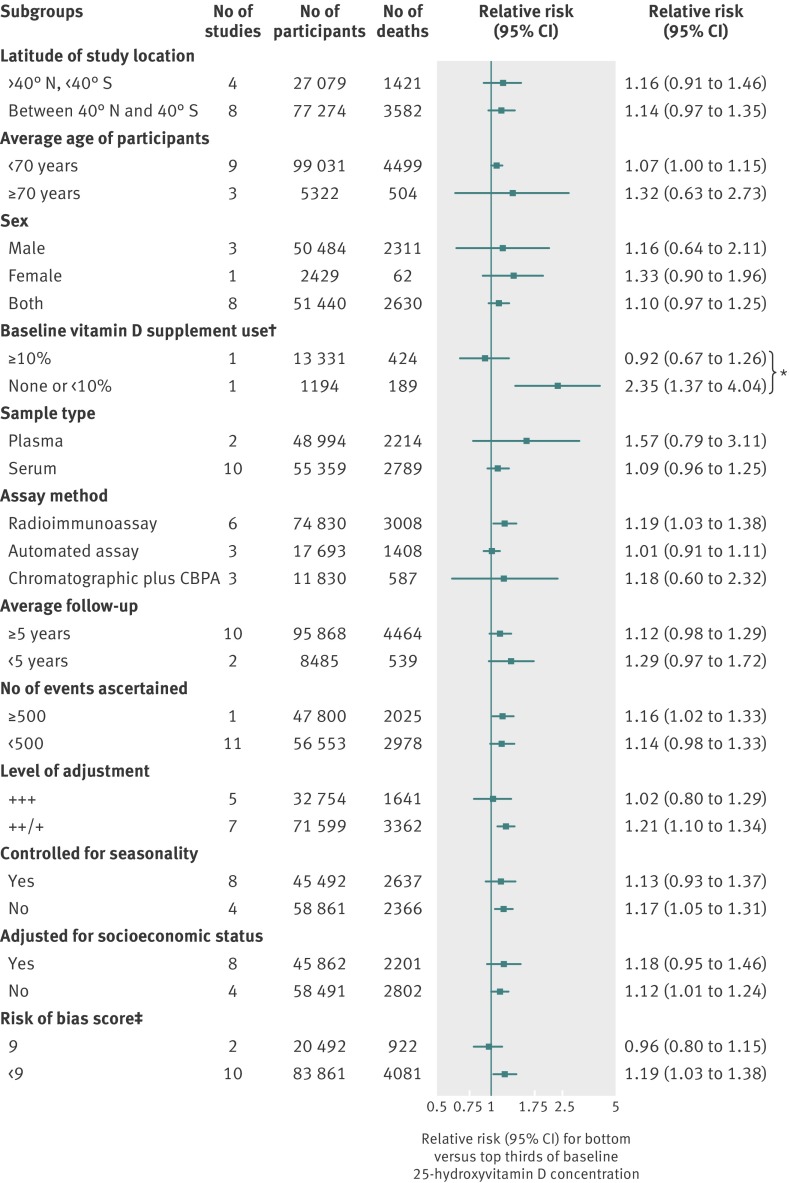
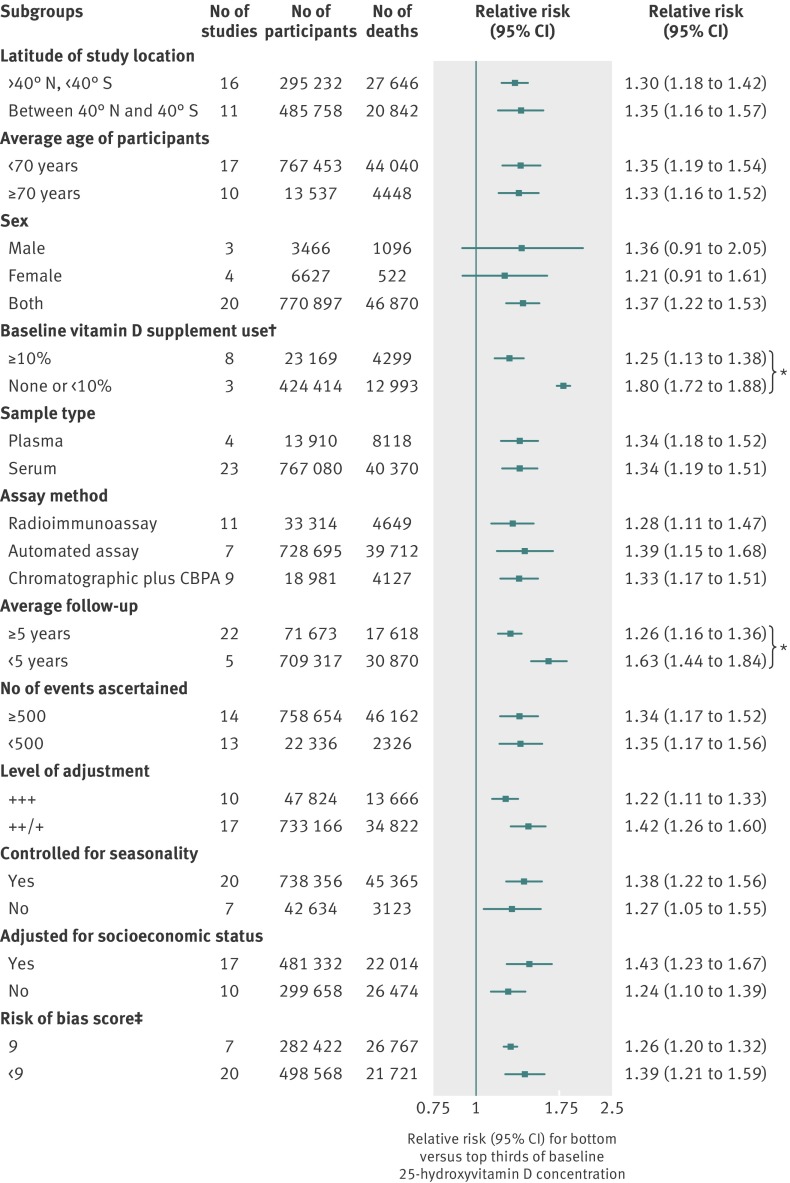
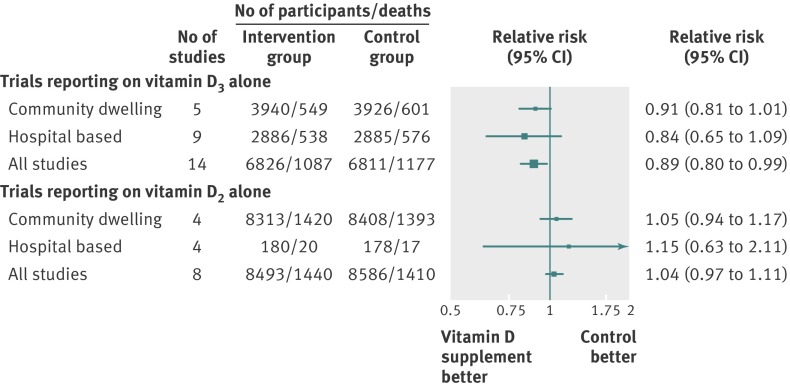
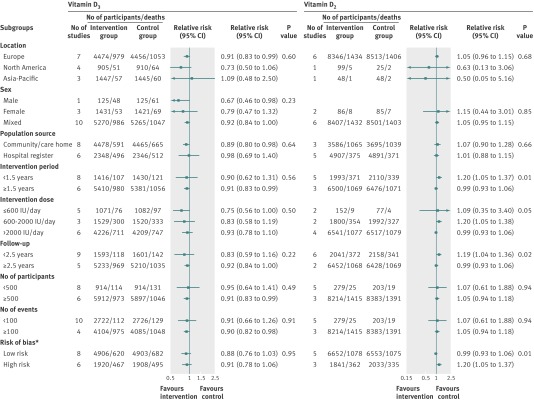
Results: In the primary prevention observational studies, comparing bottom versus top thirds of baseline circulating 25-hydroxyvitamin D distribution, pooled relative risks were 1.35 (95% confidence interval 1.13 to 1.61) for death from cardiovascular disease, 1.14 (1.01 to 1.29) for death from cancer, 1.30 (1.07 to 1.59) for non-vascular, non-cancer death, and 1.35 (1.22 to 1.49) for all cause mortality. Subgroup analyses in the observational studies indicated that risk of mortality was significantly higher in studies with lower baseline use of vitamin D supplements. In randomised controlled trials, relative risks for all cause mortality were 0.89 (0.80 to 0.99) for vitamin D3 supplementation and 1.04 (0.97 to 1.11) for vitamin D2 supplementation. The effects observed for vitamin D3 supplementation remained unchanged when grouped by various characteristics. However, for vitamin D2 supplementation, increased risks of mortality were observed in studies with lower intervention doses and shorter average intervention periods.
Conclusions: Evidence from observational studies indicates inverse associations of circulating 25-hydroxyvitamin D with risks of death due to cardiovascular disease, cancer, and other causes. Supplementation with vitamin D3 significantly reduces overall mortality among older adults; however, before any widespread supplementation, further investigations will be required to establish the optimal dose and duration and whether vitamin D3 and D2 have different effects on mortality risk.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

Comment in
-
Vitamin D and chronic disease prevention.BMJ. 2014 Apr 1;348:g2280. doi: 10.1136/bmj.g2280. BMJ. 2014. PMID: 24690627 No abstract available.
-
Vitamin D shows no clear evidence of benefits despite hundreds of studies.BMJ. 2014 Apr 1;348:g2489. doi: 10.1136/bmj.g2489. BMJ. 2014. PMID: 24692759 No abstract available.
-
Vitamin D supplements do not reduce mortality risk.BMJ. 2014 Apr 29;348:g2860. doi: 10.1136/bmj.g2860. BMJ. 2014. PMID: 24780291 No abstract available.
-
Vitamin D has a greater impact on cancer mortality rates than on cancer incidence rates.BMJ. 2014 Apr 29;348:g2862. doi: 10.1136/bmj.g2862. BMJ. 2014. PMID: 24780390 No abstract available.
-
Authors' reply to Grant and Garland and to Bolland and colleagues.BMJ. 2014 Apr 29;348:g2931. doi: 10.1136/bmj.g2931. BMJ. 2014. PMID: 24780444 No abstract available.
-
Review: vitamin D3 supplementation may reduce mortality in adults; vitamin D2 does not.Ann Intern Med. 2014 Jul 15;161(2):JC5. doi: 10.7326/0003-4819-161-2-201407150-02005. Ann Intern Med. 2014. PMID: 25023271 No abstract available.
Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Vitamin D and multiple health outcomes: umbrella review of systematic reviews and meta-analyses of observational studies and randomised trials.BMJ. 2014 Apr 1;348:g2035. doi: 10.1136/bmj.g2035. BMJ. 2014. PMID: 24690624 Free PMC article.
-
Effectiveness and safety of vitamin D in relation to bone health.Evid Rep Technol Assess (Full Rep). 2007 Aug;(158):1-235. Evid Rep Technol Assess (Full Rep). 2007. PMID: 18088161 Free PMC article. Review.
-
Vitamin D supplementation in pregnancy: a systematic review.Health Technol Assess. 2014 Jul;18(45):1-190. doi: 10.3310/hta18450. Health Technol Assess. 2014. PMID: 25025896 Free PMC article. Review.
-
Association between vitamin D supplementation and mortality: systematic review and meta-analysis.BMJ. 2019 Aug 12;366:l4673. doi: 10.1136/bmj.l4673. BMJ. 2019. PMID: 31405892 Free PMC article.
Cited by
-
Estimation of the optimum dose of vitamin D for disease prevention in older people: rationale, design and baseline characteristics of the BEST-D trial.Maturitas. 2015 Apr;80(4):426-31. doi: 10.1016/j.maturitas.2015.01.013. Epub 2015 Feb 7. Maturitas. 2015. PMID: 25721698 Free PMC article. Clinical Trial.
-
Vitamin D Receptor Polymorphisms Are Associated with Reduced Esophageal Vitamin D Receptor Expression and Reduced Esophageal Adenocarcinoma Risk.Mol Med. 2015 Apr 21;21(1):346-54. doi: 10.2119/molmed.2012.00336. Mol Med. 2015. PMID: 25910066 Free PMC article.
-
The effect on quality of life of vitamin D administration for advanced cancer treatment (VIDAFACT study): protocol of a randomised controlled trial.BMJ Open. 2014 Dec 31;4(12):e006128. doi: 10.1136/bmjopen-2014-006128. BMJ Open. 2014. PMID: 25552610 Free PMC article. Clinical Trial.
-
The association between serum 25-hydroxyvitamin D level and recurrent falls in the elderly population: a cohort study.Electron Physician. 2016 Aug 25;8(8):2707-2712. doi: 10.19082/2707. eCollection 2016 Aug. Electron Physician. 2016. PMID: 27757178 Free PMC article.
-
Vitamin D Status and Long-Term Mortality in Community-Acquired Pneumonia: Secondary Data Analysis from a Prospective Cohort.PLoS One. 2016 Jul 1;11(7):e0158536. doi: 10.1371/journal.pone.0158536. eCollection 2016. PLoS One. 2016. PMID: 27367810 Free PMC article.
References
-
- Holick MF. Vitamin D: physiology, dietary sources and requirements. In: Encyclopedia of human nutrition. 2nd ed. Academic Press, 2005.
-
- Holick MF. Vitamin D deficiency. N Engl J Med 2007;357:266-81. - PubMed
-
- Bischoff-Ferrari HA, Willett WC, Orav EJ, Lips P, Meunier PJ, Lyons RA, et al. A pooled analysis of vitamin D dose requirements for fracture prevention. N Engl J Med 2012;367:40-9. - PubMed
-
- Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Staehelin HB, Bazemore MG, Zee RY, et al. Effect of vitamin D on falls: a meta-analysis. JAMA 2004;291:1999-2006. - PubMed
-
- Winzenberg TM, Powell S, Shaw KA, Jones G. Vitamin D supplementation for improving bone mineral density in children. Cochrane Database Syst Rev 2010;(10):CD006944. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical