

HCMV infection of human trophoblast progenitor cells of the placenta is neutralized by a human monoclonal antibody to glycoprotein B and not by antibodies to the pentamer complex
- PMID: 24651029
- PMCID: PMC3970154
- DOI: 10.3390/v6031346
HCMV infection of human trophoblast progenitor cells of the placenta is neutralized by a human monoclonal antibody to glycoprotein B and not by antibodies to the pentamer complex
Abstract
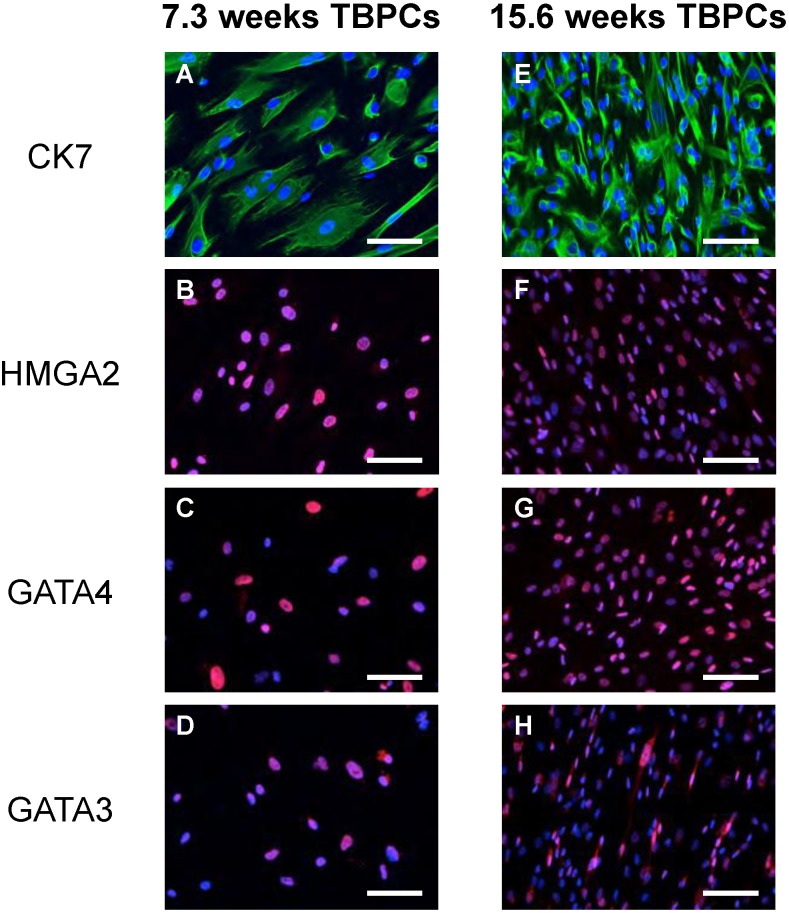
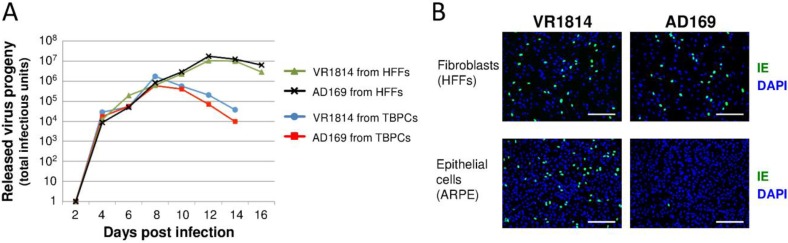
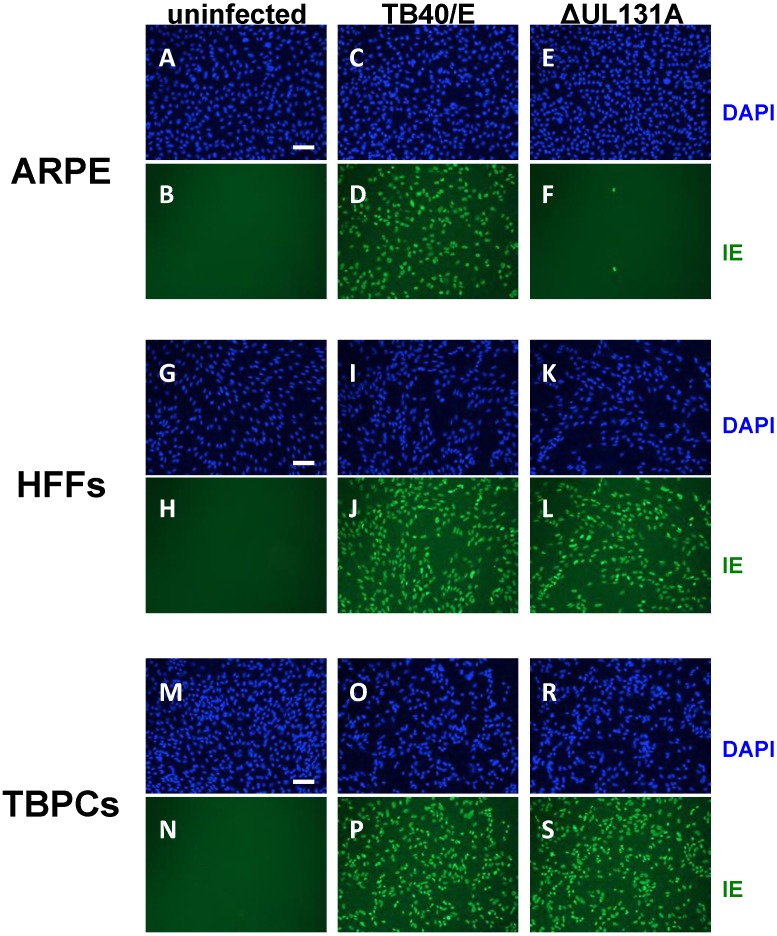
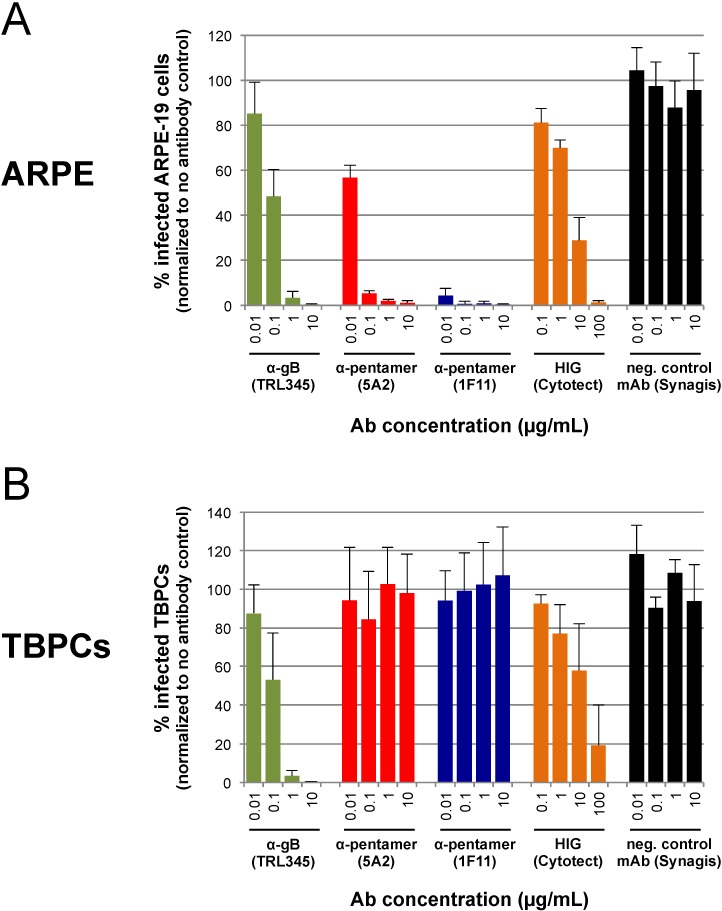
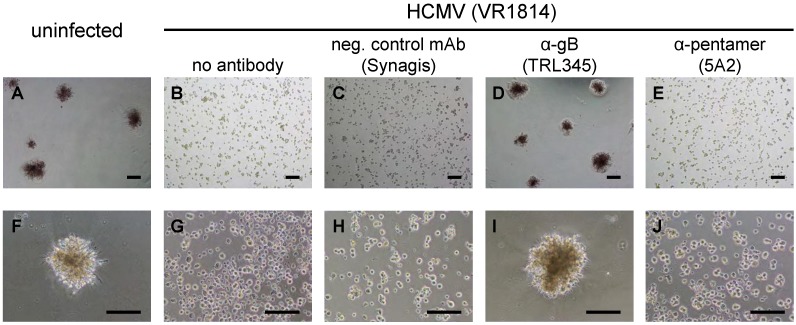
Human cytomegalovirus (HCMV) is the major viral cause of congenital infection and birth defects. Primary maternal infection often results in virus transmission, and symptomatic babies can have permanent neurological deficiencies and deafness. Congenital infection can also lead to intrauterine growth restriction, a defect in placental transport. HCMV replicates in primary cytotrophoblasts (CTBs), the specialized cells of the placenta, and inhibits differentiation/invasion. Human trophoblast progenitor cells (TBPCs) give rise to the mature cell types of the chorionic villi, CTBs and multi-nucleated syncytiotrophoblasts (STBs). Here we report that TBPCs are fully permissive for pathogenic and attenuated HCMV strains. Studies with a mutant virus lacking a functional pentamer complex (gH/gL/pUL128-131A) showed that virion entry into TBPCs is independent of the pentamer. In addition, infection is blocked by a potent human neutralizing monoclonal antibody (mAb), TRL345, reactive with glycoprotein B (gB), but not mAbs to the pentamer proteins pUL130/pUL131A. Functional studies revealed that neutralization of infection preserved the capacity of TBPCs to differentiate and assemble into trophospheres composed of CTBs and STBs in vitro. Our results indicate that mAbs to gB protect trophoblast progenitors of the placenta and could be included in antibody treatments developed to suppress congenital infection and prevent disease.
Figures

Similar articles
-
Human cytomegalovirus infection interferes with the maintenance and differentiation of trophoblast progenitor cells of the human placenta.J Virol. 2015 May;89(9):5134-47. doi: 10.1128/JVI.03674-14. Epub 2015 Mar 4. J Virol. 2015. PMID: 25741001 Free PMC article.
-
Monoclonal Antibodies to Different Components of the Human Cytomegalovirus (HCMV) Pentamer gH/gL/pUL128L and Trimer gH/gL/gO as well as Antibodies Elicited during Primary HCMV Infection Prevent Epithelial Cell Syncytium Formation.J Virol. 2016 Jun 24;90(14):6216-6223. doi: 10.1128/JVI.00121-16. Print 2016 Jul 15. J Virol. 2016. PMID: 27122579 Free PMC article.
-
Vaccine-Derived Neutralizing Antibodies to the Human Cytomegalovirus gH/gL Pentamer Potently Block Primary Cytotrophoblast Infection.J Virol. 2015 Dec;89(23):11884-98. doi: 10.1128/JVI.01701-15. Epub 2015 Sep 16. J Virol. 2015. PMID: 26378171 Free PMC article.
-
Congenital cytomegalovirus infection undermines early development and functions of the human placenta.Placenta. 2017 Nov;59 Suppl 1:S8-S16. doi: 10.1016/j.placenta.2017.04.020. Epub 2017 Apr 25. Placenta. 2017. PMID: 28477968 Review.
-
Pathogen at the Gates: Human Cytomegalovirus Entry and Cell Tropism.Viruses. 2018 Dec 11;10(12):704. doi: 10.3390/v10120704. Viruses. 2018. PMID: 30544948 Free PMC article. Review.
Cited by
-
Intrauterine Fetal Demise, Spontaneous Abortion and Congenital Cytomegalovirus: A Systematic Review of the Incidence and Histopathologic Features.Viruses. 2024 Sep 30;16(10):1552. doi: 10.3390/v16101552. Viruses. 2024. PMID: 39459885 Free PMC article.
-
Human cytomegalovirus infection interferes with the maintenance and differentiation of trophoblast progenitor cells of the human placenta.J Virol. 2015 May;89(9):5134-47. doi: 10.1128/JVI.03674-14. Epub 2015 Mar 4. J Virol. 2015. PMID: 25741001 Free PMC article.
-
Role of pentamer complex-specific and IgG subclass 3 antibodies in HCMV hyperimmunoglobulin and standard intravenous IgG preparations.Med Microbiol Immunol. 2019 Feb;208(1):69-80. doi: 10.1007/s00430-018-0558-x. Epub 2018 Sep 10. Med Microbiol Immunol. 2019. PMID: 30203132
-
Development of novel vaccines against human cytomegalovirus.Hum Vaccin Immunother. 2019;15(11):2673-2683. doi: 10.1080/21645515.2019.1593729. Epub 2019 Apr 24. Hum Vaccin Immunother. 2019. PMID: 31017831 Free PMC article. Review.
-
Identification of a neutralizing epitope within antigenic domain 5 of glycoprotein B of human cytomegalovirus.J Virol. 2015 Jan;89(1):361-72. doi: 10.1128/JVI.02393-14. Epub 2014 Oct 15. J Virol. 2015. PMID: 25320309 Free PMC article.
References
-
- Britt W.J. Congenital cytomegalovirus infection. In: Hitchcock P.J., MacKay H.T., Wasserheit J.N., editors. Sexually Transmitted Diseases and Adverse Outcomes of Pregnancy. ASM Press; Washington, DC, USA: 1999. pp. 269–281.
-
- Demmler G.J. Congenital cytomegalovirus infection and disease. Adv. Pediatr. Infect. Dis. 1996;11:135–162. - PubMed
-
- Fowler K.B., Stagno S., Pass R.F. Maternal immunity and prevention of congenital cytomegalovirus infection. JAMA. 2003;289:1008–1011. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
