

Gallbladder cancer: epidemiology and outcome
- PMID: 24634588
- PMCID: PMC3952897
- DOI: 10.2147/CLEP.S37357
Gallbladder cancer: epidemiology and outcome
Abstract
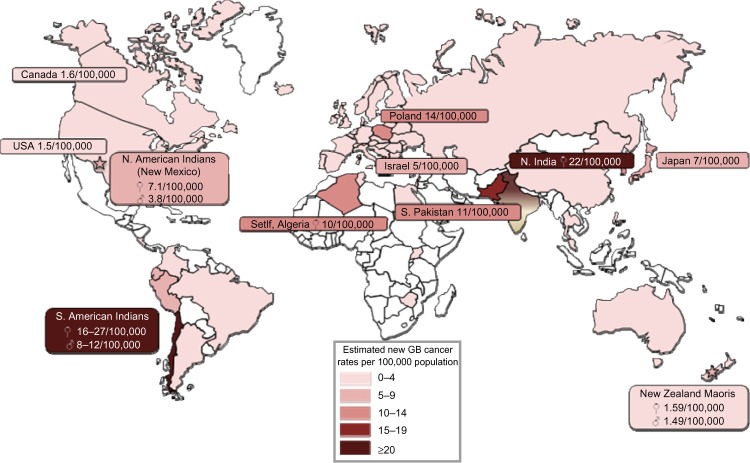
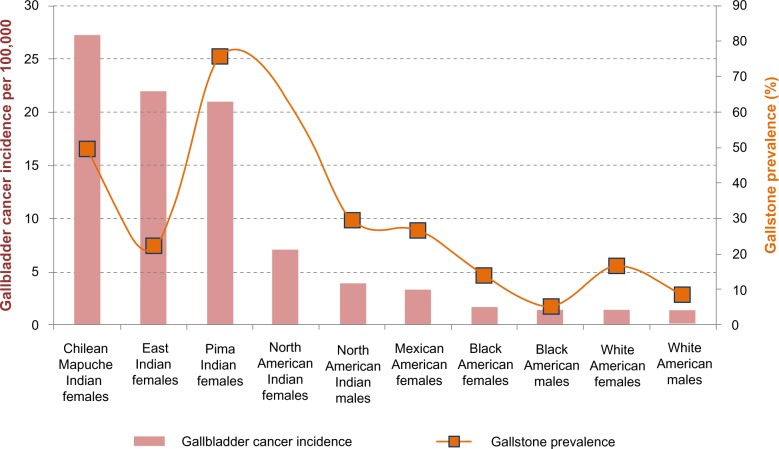
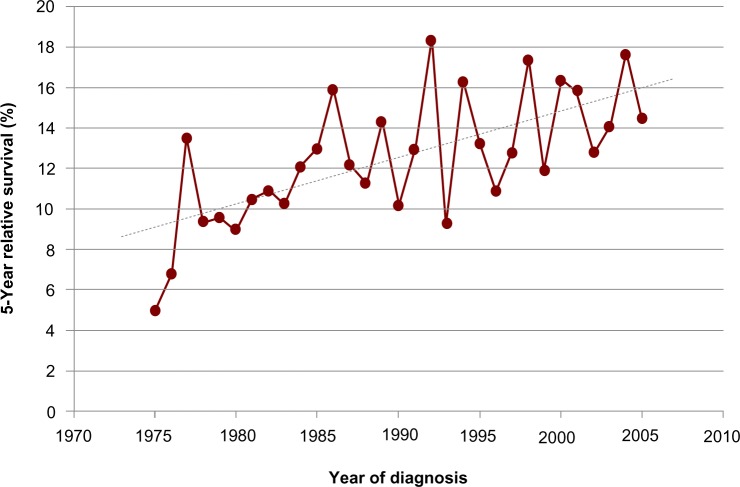
Gallbladder cancer, though generally considered rare, is the most common malignancy of the biliary tract, accounting for 80%-95% of biliary tract cancers. An early diagnosis is essential as this malignancy progresses silently with a late diagnosis, often proving fatal. Its carcinogenesis follows a progression through a metaplasia-dysplasia-carcinoma sequence. This comprehensive review focuses on and explores the risks, management, and outcomes for primary gallbladder carcinoma. Epidemiological studies have identified striking geographic and ethnic disparities - inordinately high occurrence in American Indians, elevated in Southeast Asia, yet quite low elsewhere in the Americas and the world. Age, female sex, congenital biliary tract anomalies, and a genetic predisposition represent important risk factors that are immutable. Environmental triggers play a critical role in eliciting cancer developing in the gallbladder, best exemplified by cholelithiasis and chronic inflammation from biliary tract and parasitic infections. Mortality rates closely follow incidence; those countries with the highest prevalence of gallstones experience the greatest mortality from gallbladder cancer. Vague symptoms often delay the diagnosis of gallbladder cancer, contributing to its overall progression and poor outcome. Surgery represents the only potential for cure. Some individuals are fortunate to be incidentally found to have gallbladder cancer at the time of cholecystectomy being performed for cholelithiasis. Such an early diagnosis is imperative as a late presentation connotes advanced staging, nodal involvement, and possible recurrence following attempted resection. Overall mean survival is a mere 6 months, while 5-year survival rate is only 5%. The dismal prognosis, in part, relates to the gallbladder lacking a serosal layer adjacent to the liver, enabling hepatic invasion and metastatic progression. Improved imaging modalities are helping to diagnose patients at an earlier stage. The last decade has witnessed improved outcomes as aggressive surgical management and preoperative adjuvant therapy has helped prolong survival in patients with gallbladder cancer. In the future, the development of potential diagnostic markers for disease will yield screening opportunities for those at risk either with ethnic susceptibility or known anatomic anomalies of the biliary tract. Meanwhile, clarification of the value of prophylactic cholecystectomy should provide an opportunity for secondary prevention. Primary prevention will arrive once the predictive biomarkers and environmental risk factors are more clearly identified.
Keywords: anomalous junction of the pancreaticobiliary duct; cholecystectomy; cholelithiasis; gallbladder polyp; gallstones; incidence; primary sclerosing cholangitis.
Figures

Similar articles
-
Gallbladder cancer.Hepatobiliary Surg Nutr. 2014 Oct;3(5):221-6. doi: 10.3978/j.issn.2304-3881.2014.09.03. Hepatobiliary Surg Nutr. 2014. PMID: 25392833 Free PMC article. Review.
-
Risk factors for biliary tract and ampullary carcinomas and prophylactic surgery for these factors.J Hepatobiliary Pancreat Surg. 2008;15(1):15-24. doi: 10.1007/s00534-007-1276-8. Epub 2008 Feb 16. J Hepatobiliary Pancreat Surg. 2008. PMID: 18274840 Free PMC article. Review.
-
Primary gallbladder cancer: recognition of risk factors and the role of prophylactic cholecystectomy.Am J Gastroenterol. 2000 Jun;95(6):1402-10. doi: 10.1111/j.1572-0241.2000.02070.x. Am J Gastroenterol. 2000. PMID: 10894571
-
Gallbladder carcinoma with biliary invasion: clinical analysis of the differences from nonbiliary invasion.World J Surg. 2005 Jan;29(1):72-5. doi: 10.1007/s00268-004-7544-8. World J Surg. 2005. PMID: 15599737
-
A Review of the Etiology and Epidemiology of Gallbladder Cancer: What You Need to Know.Cureus. 2022 Aug 22;14(8):e28260. doi: 10.7759/cureus.28260. eCollection 2022 Aug. Cureus. 2022. PMID: 36158346 Free PMC article. Review.
Cited by
-
Associations between external beam radiotherapy and overall survival in patients with gallbladder cancer: A population-based study.Front Public Health. 2022 Oct 10;10:1012142. doi: 10.3389/fpubh.2022.1012142. eCollection 2022. Front Public Health. 2022. PMID: 36311614 Free PMC article.
-
Prognostic Nomograms to Predict Survival of Patients with Resectable Gallbladder Cancer: A Surveillance, Epidemiology, and End Results (SEER)-Based Analysis.Med Sci Monit. 2021 Mar 30;27:e929106. doi: 10.12659/MSM.929106. Med Sci Monit. 2021. PMID: 33784268 Free PMC article.
-
Role of EGFR and HER-2/NEU Expression in Gall Bladder Carcinoma (GBC).J Lab Physicians. 2021 Mar;13(1):29-35. doi: 10.1055/s-0041-1726561. Epub 2021 May 19. J Lab Physicians. 2021. PMID: 34103877 Free PMC article.
-
RNA sequencing-based analysis of gallbladder cancer reveals the importance of the liver X receptor and lipid metabolism in gallbladder cancer.Oncotarget. 2016 Jun 7;7(23):35302-12. doi: 10.18632/oncotarget.9181. Oncotarget. 2016. PMID: 27167107 Free PMC article.
-
PD-1 inhibitors plus nab-paclitaxel-containing chemotherapy for advanced gallbladder cancer in a second-line setting: A retrospective analysis of a case series.Front Oncol. 2022 Nov 16;12:1006075. doi: 10.3389/fonc.2022.1006075. eCollection 2022. Front Oncol. 2022. PMID: 36465365 Free PMC article.
References
-
- Lazcano-Ponce EC, Miquel JF, Muñoz N, et al. Epidemiology and molecular pathology of gallbladder cancer. CA: Cancer J Clin 2001. 2001;51(6):349–364. - PubMed
-
- Sheth S, Bedford A, Chopra S. Primary gallbladder cancer: recognition of risk factors and the role of prophylactic cholecystectomy. Am J Gastroenterol. 2000;95(6):1402–1410. - PubMed
-
- Duffy A, Capanu M, Abou-Alfa GK, et al. Gallbladder cancer (GBC): 10-year experience at Memorial Sloan-Kettering Cancer Centre (MSKCC) J Surg Oncol. 2008;98(7):485–489. - PubMed
-
- Levy AD, Murakata LA, Rohrmann CA., Jr Gallbladder carcinoma: radiologic-pathologic correlation. Radiographics. 2001;21(2):295–314. questionnaire, 549–555. - PubMed
-
- Wistuba II, Gazdar AF. Gallbladder cancer: lessons from a rare tumour. Nat Rev Cancer. 2004;4(9):695–706. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
