

The association of the 'additional height index' with atopic diseases, non-atopic asthma, ischaemic heart disease and mortality: a population-based study
- PMID: 24583759
- PMCID: PMC3939652
- DOI: 10.1136/bmjopen-2013-003933
The association of the 'additional height index' with atopic diseases, non-atopic asthma, ischaemic heart disease and mortality: a population-based study
Abstract
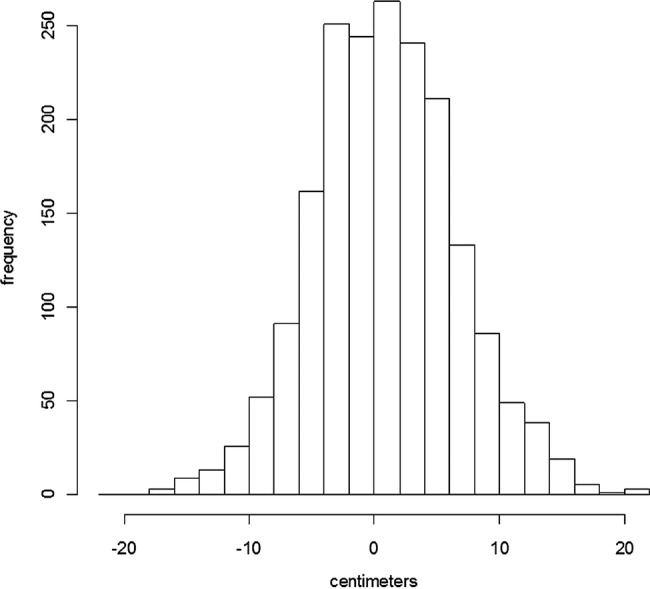
Objective: Intrauterine growth has been associated with atopic conditions. Growth and adult height have been associated with cardiovascular disease, cancers and mortality but are highly genetic traits. The objectives of the study were as follows: first, to define a height measure indicating an individual's height below or above that which could be expected based on parental height (genetic inheritance) and growth charts. It was named 'the additional height index' (AHI), defined as (attained-expected) height; second, to investigate possible associations of AHI with atopic versus non-atopic health outcomes and with ischaemic heart disease (IHD) and IHD mortality.
Design: General population-based study.
Setting: Research centre.
Participants: A random sample of 2656 men and women living in greater Copenhagen took part in the MONICA10 study (the Danish monitoring trends and determinants of cardiovascular disease). In total, 1900 participants with information of parental height were selected.
Outcome measures: Atopic sensitisation (serum IgE), questionnaire information of atopic dermatitis, rhinoconjunctivitis, asthma or wheezing, and registry-based diagnoses of IHD/IHD mortality from National Registries.
Results: Increasing levels of AHI were inversely associated with non-atopic asthma, non-atopic wheezing, IHD and IHD mortality (IHD-all). For one SD increase of AHI, the OR or HR with CI in adjusted analyses was non-atopic asthma OR=0.52 (0.36 to 0.74), non-atopic wheezing OR=0.67 (0.51 to 0.89), and IHD-all HR=0.89 (0.78 to 1.01). The level of AHI was higher among individuals with atopic dermatitis, allergic rhinoconjunctivitis and atopic sensitisation (all p values <0.001) compared with individuals without those conditions; however, the associations were not confirmed in adjusted analyses.
Conclusions: Individuals with childhood conditions that led them to attain tallness higher than expected from their parents' height may be at lower risk of non-atopic asthma/wheeze and IHD/IHD mortality but possibly at higher risk of atopic conditions. The measure of tallness below or above the expected height could be a sensitive alternative to normal height in epidemiological analyses.
Figures


Similar articles
-
Prevention of allergic disease in childhood: clinical and epidemiological aspects of primary and secondary allergy prevention.Pediatr Allergy Immunol. 2004 Jun;15 Suppl 16:4-5, 9-32. doi: 10.1111/j.1399-3038.2004.0148b.x. Pediatr Allergy Immunol. 2004. PMID: 15125698 Review.
-
Associations of maternal atopic diseases with adverse pregnancy outcomes: a national cohort study.Paediatr Perinat Epidemiol. 2014 Nov;28(6):489-97. doi: 10.1111/ppe.12154. Epub 2014 Oct 30. Paediatr Perinat Epidemiol. 2014. PMID: 25359226 Free PMC article.
-
The validity of register data to identify children with atopic dermatitis, asthma or allergic rhinoconjunctivitis.Pediatr Allergy Immunol. 2017 Sep;28(6):535-542. doi: 10.1111/pai.12743. Epub 2017 Jul 27. Pediatr Allergy Immunol. 2017. PMID: 28632331
-
Incidence rates of atopic dermatitis, asthma, and allergic rhinoconjunctivitis in Danish and Swedish children.J Allergy Clin Immunol. 2015 Aug;136(2):360-6.e2. doi: 10.1016/j.jaci.2015.02.003. Epub 2015 Mar 29. J Allergy Clin Immunol. 2015. PMID: 25828267
-
The burden of atopy and asthma in children.Allergy. 2004 Aug;59 Suppl 78:7-11. doi: 10.1111/j.1398-9995.2004.00563.x. Allergy. 2004. PMID: 15245350 Review.
Cited by
-
Comparison of two automated assays of BTM (CTX and P1NP) and reference intervals in a Danish population.Osteoporos Int. 2017 Jul;28(7):2103-2113. doi: 10.1007/s00198-017-4026-z. Epub 2017 Apr 28. Osteoporos Int. 2017. PMID: 28455749
References
-
- von Hertzen LC, Haahtela T. Asthma and atopy—the price of affluence? Allergy 2004;59:124–37 - PubMed
-
- Linneberg A, Nielsen NH, Madsen F, et al. Secular trends of allergic asthma in Danish adults. The Copenhagen Allergy Study. Respir Med 2001;95:258–64 - PubMed
-
- Umetsu DT, McIntire JJ, Akbari O, et al. Asthma: an epidemic of dysregulated immunity. Nat Immunol 2002;3:715–20 - PubMed
-
- Bjorksten B, Clayton T, Ellwood P, et al. Worldwide time trends for symptoms of rhinitis and conjunctivitis: Phase III of the International Study of Asthma and Allergies in Childhood. Pediatr Allergy Immunol 2008;19:110–24 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical