

Assessment of myocardial viability and left ventricular function in patients supported by a left ventricular assist device
- PMID: 24582837
- PMCID: PMC3966997
- DOI: 10.1016/j.healun.2014.01.866
Assessment of myocardial viability and left ventricular function in patients supported by a left ventricular assist device
Abstract
Background: Chronically supported left ventricular assist device (LVAD) patients may be candidates for novel therapies aimed at promoting reverse remodeling and myocardial recovery. However, the effect of hemodynamic unloading with a LVAD on myocardial viability and LV function in chronically supported LVAD patients has not been fully characterized. We aimed to develop a non-invasive imaging protocol to serially quantify native cardiac structure, function, and myocardial viability while at reduced LVAD support.
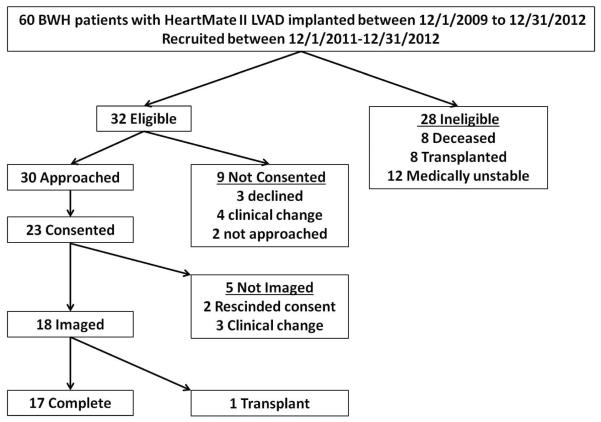
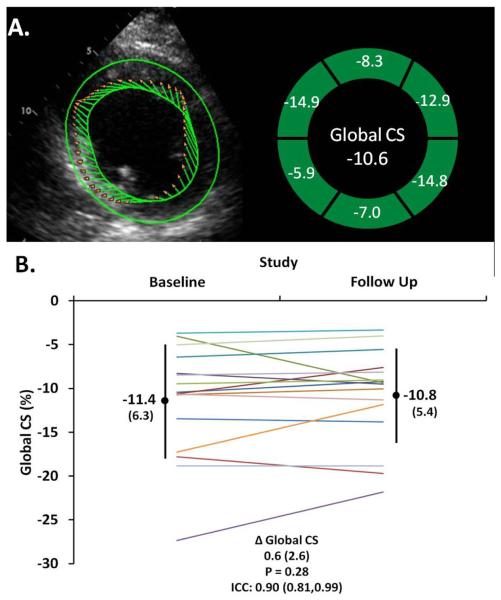
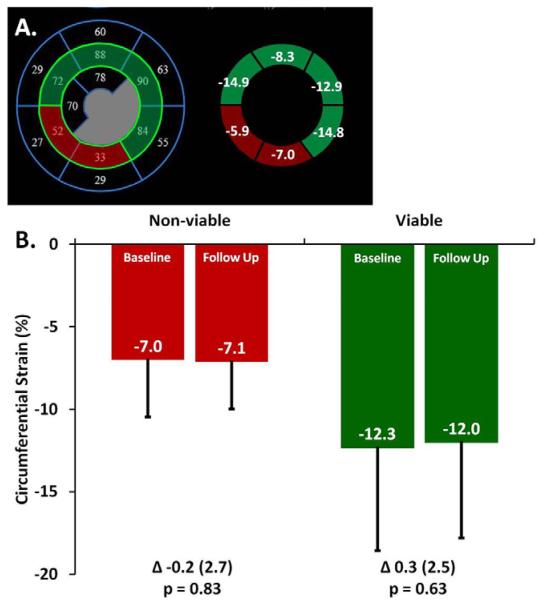
Methods: Clinically stable (n = 18) ambulatory patients (83% men, median age, 61 years) supported by a HeartMate II (Thoratec, Pleasanton, CA) LVAD (median durations of heart failure 4.6 years and LVAD support 7 months) were evaluated by echocardiography and technetium-99m ((99m)Tc)-sestamibi single photon emission computed tomography (SPECT) imaging at baseline and after an interval of 2 to 3 months. Echocardiographic measures of LV size and function, including speckle tracking-derived circumferential strain, were compared between ambulatory and reduced LVAD support at baseline and between baseline and follow-up at reduced LVAD support. The extent of myocardial viability by SPECT was compared between baseline and follow-up at reduced LVAD support.
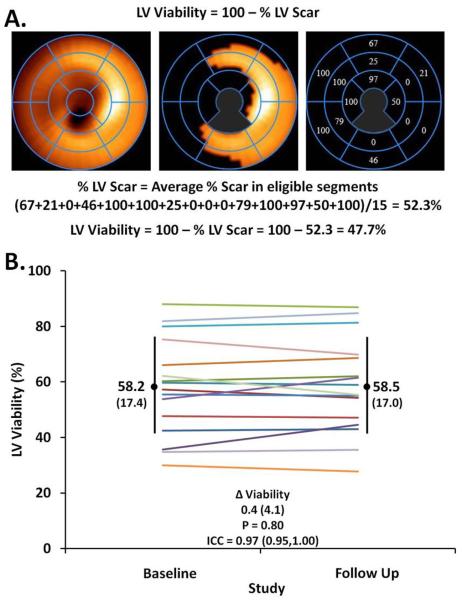
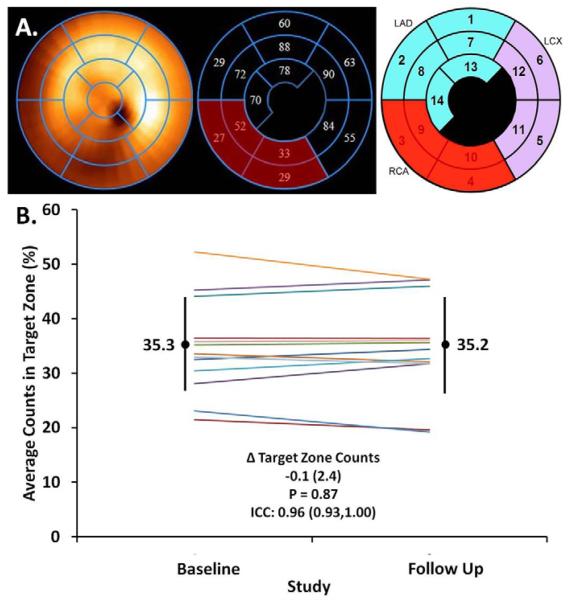
Results: With reduction in LVAD speeds (6,600 rpm; interquartile range: 6,200, 7,400 rpm), LV size increased, LV systolic function remained stable, and filling pressures nominally worsened. After a median 2.1 months, cardiac structure, function, and the extent of viable myocardium, globally and regionally, was unchanged on repeat imaging while at reduced LVAD speed.
Conclusions: In clinically stable chronically supported LVAD patients, intrinsic cardiac structure, function, and myocardial viability did not significantly change over the pre-specified time frame. Echocardiographic circumferential strain and (99m)Tc-sestamibi SPECT myocardial viability imaging may provide useful non-invasive end points for the assessment of cardiac structure and function, particularly for phase II studies of novel therapies aimed at promoting reverse remodeling and myocardial recovery in LVAD patients.
Keywords: hemodynamic unloading; left ventricular assist device; reverse remodeling; single photon emission computed tomography; speckle tracking echocardiography.
Copyright © 2014 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Myocardial atrophy and chronic mechanical unloading of the failing human heart: implications for cardiac assist device-induced myocardial recovery.J Am Coll Cardiol. 2014 Oct 14;64(15):1602-12. doi: 10.1016/j.jacc.2014.05.073. J Am Coll Cardiol. 2014. PMID: 25301465
-
Novel Left Heart Catheterization Ramp Protocol to Guide Hemodynamic Optimization in Patients Supported With Left Ventricular Assist Device Therapy.J Am Heart Assoc. 2019 Feb 19;8(4):e010232. doi: 10.1161/JAHA.118.010232. J Am Heart Assoc. 2019. PMID: 30755070 Free PMC article.
-
Prospective Multicenter Study of Myocardial Recovery Using Left Ventricular Assist Devices (RESTAGE-HF [Remission from Stage D Heart Failure]): Medium-Term and Primary End Point Results.Circulation. 2020 Nov 24;142(21):2016-2028. doi: 10.1161/CIRCULATIONAHA.120.046415. Epub 2020 Oct 26. Circulation. 2020. PMID: 33100036
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
-
The Effect of Left Ventricular Assist Device Therapy on Cardiac Biomarkers: Implications for the Identification of Myocardial Recovery.Curr Heart Fail Rep. 2018 Aug;15(4):250-259. doi: 10.1007/s11897-018-0399-3. Curr Heart Fail Rep. 2018. PMID: 29971612 Review.
Cited by
-
Myocardial Recovery.Diagnostics (Basel). 2023 Apr 21;13(8):1504. doi: 10.3390/diagnostics13081504. Diagnostics (Basel). 2023. PMID: 37189604 Free PMC article. Review.
-
Role of Echocardiography in the Management of Patients with Advanced (Stage D) Heart Failure Related to Nonischemic Cardiomyopathy.Rev Cardiovasc Med. 2022 Jun 15;23(6):214. doi: 10.31083/j.rcm2306214. eCollection 2022 Jun. Rev Cardiovasc Med. 2022. PMID: 39077176 Free PMC article. Review.
-
Expanding the Scope of Multimodality Imaging in Durable Mechanical Circulatory Support.JACC Cardiovasc Imaging. 2020 Apr;13(4):1069-1081. doi: 10.1016/j.jcmg.2019.05.035. Epub 2019 Sep 18. JACC Cardiovasc Imaging. 2020. PMID: 31542528 Free PMC article. Review.
-
Weaning from ventricular assist device support after recovery from left ventricular failure with or without secondary right ventricular failure.Cardiovasc Diagn Ther. 2021 Feb;11(1):226-242. doi: 10.21037/cdt-20-288. Cardiovasc Diagn Ther. 2021. PMID: 33708495 Free PMC article. Review.
-
Role of Echocardiography in the Evaluation of Left Ventricular Assist Devices: the Importance of Emerging Technologies.Curr Cardiol Rep. 2016 Jul;18(7):62. doi: 10.1007/s11886-016-0739-4. Curr Cardiol Rep. 2016. PMID: 27216842 Review.
References
-
- Kirklin JK, Naftel DC, Kormos RL, et al. Fifth INTERMACS annual report: risk factor analysis from more than 6,000 mechanical circulatory support patients. J Heart Lung Transplant. 2013;32:141–56. - PubMed
-
- Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. 2001;345:1435–43. - PubMed
-
- Miller LW, Pagani FD, Russell SD, et al. Use of a continuous-flow device in patients awaiting heart transplantation. N Engl J Med. 2007;357:885–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
