

Constitutive activation of PKA catalytic subunit in adrenal Cushing's syndrome
- PMID: 24571724
- PMCID: PMC4727447
- DOI: 10.1056/NEJMoa1310359
Constitutive activation of PKA catalytic subunit in adrenal Cushing's syndrome
Abstract
Background: Corticotropin-independent Cushing's syndrome is caused by tumors or hyperplasia of the adrenal cortex. The molecular pathogenesis of cortisol-producing adrenal adenomas is not well understood.
Methods: We performed exome sequencing of tumor-tissue specimens from 10 patients with cortisol-producing adrenal adenomas and evaluated recurrent mutations in candidate genes in an additional 171 patients with adrenocortical tumors. We also performed genomewide copy-number analysis in 35 patients with cortisol-secreting bilateral adrenal hyperplasias. We studied the effects of these genetic defects both clinically and in vitro.
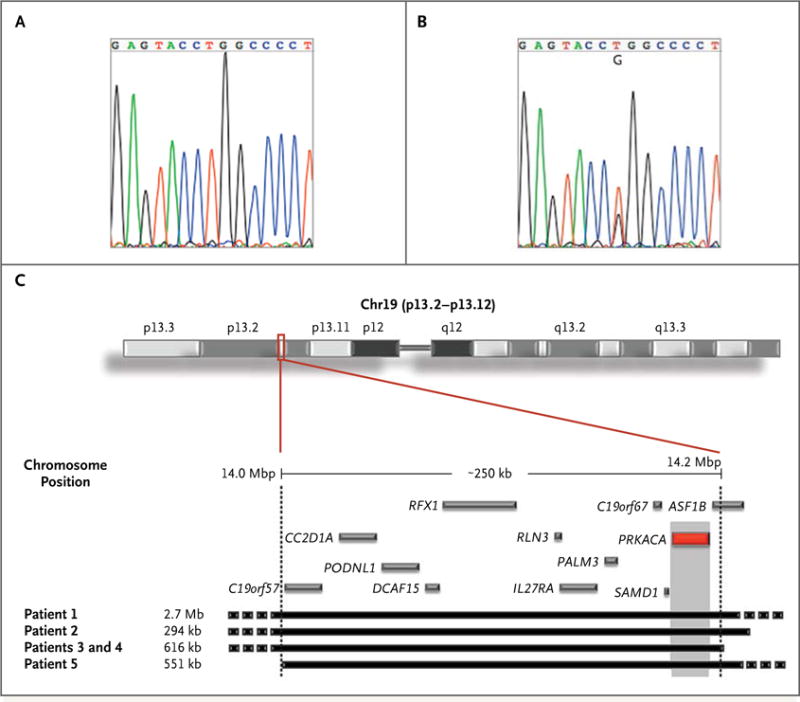
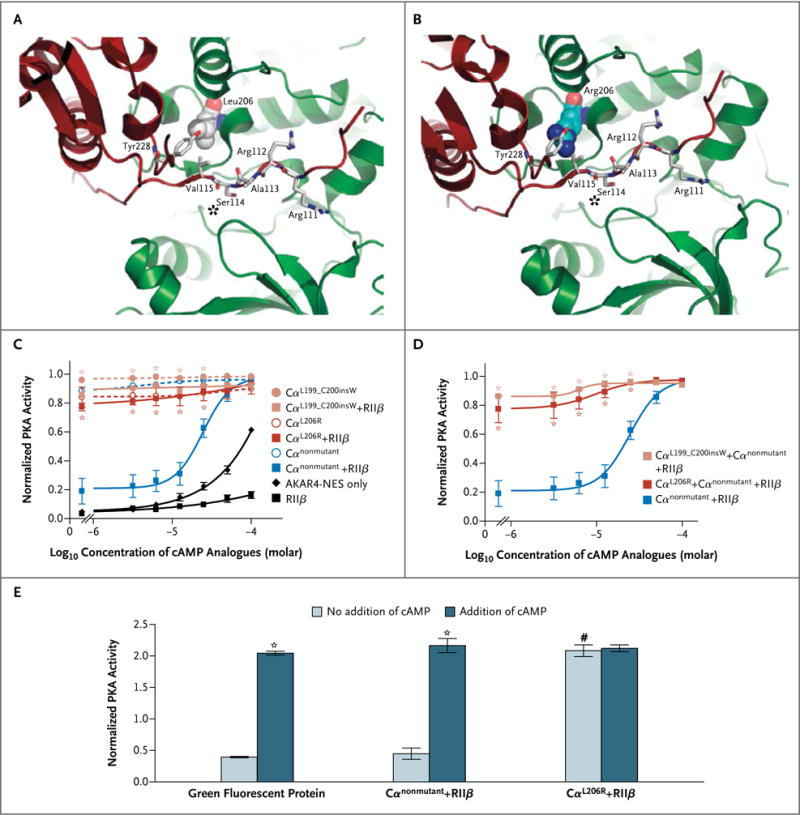
Results: Exome sequencing revealed somatic mutations in PRKACA, which encodes the catalytic subunit of cyclic AMP-dependent protein kinase (protein kinase A [PKA]), in 8 of 10 adenomas (c.617A→C in 7 and c.595_596insCAC in 1). Overall, PRKACA somatic mutations were identified in 22 of 59 unilateral adenomas (37%) from patients with overt Cushing's syndrome; these mutations were not detectable in 40 patients with subclinical hypercortisolism or in 82 patients with other adrenal tumors. Among 35 patients with cortisol-producing hyperplasias, 5 (including 2 first-degree relatives) carried a germline copy-number gain (duplication) of the genomic region on chromosome 19 that includes PRKACA. In vitro studies showed impaired inhibition of both PKA catalytic subunit mutants by the PKA regulatory subunit, whereas cells from patients with germline chromosomal gains showed increased protein levels of the PKA catalytic subunit; in both instances, basal PKA activity was increased.
Conclusions: Genetic alterations of the catalytic subunit of PKA were found to be associated with human disease. Germline duplications of this gene resulted in bilateral adrenal hyperplasias, whereas somatic PRKACA mutations resulted in unilateral cortisol-producing adrenal adenomas. (Funded by the European Commission Seventh Framework Program and others.).
Figures
Comment in
-
Genetics: Pinpointing a hotspot in adrenal Cushing syndrome.Nat Rev Endocrinol. 2014 Aug;10(8):447-8. doi: 10.1038/nrendo.2014.89. Epub 2014 Jun 10. Nat Rev Endocrinol. 2014. PMID: 24913521 No abstract available.
Similar articles
-
Somatic mutations of the catalytic subunit of cyclic AMP-dependent protein kinase (PRKACA) gene in Japanese patients with several adrenal adenomas secreting cortisol [Rapid Communication].Endocr J. 2014;61(8):825-32. doi: 10.1507/endocrj.ej14-0282. Epub 2014 Jul 25. Endocr J. 2014. PMID: 25069672
-
PRKACA mutations in cortisol-producing adenomas and adrenal hyperplasia: a single-center study of 60 cases.Eur J Endocrinol. 2015 Jun;172(6):677-85. doi: 10.1530/EJE-14-1113. Epub 2015 Mar 6. Eur J Endocrinol. 2015. PMID: 25750087
-
Novel somatic mutations in the catalytic subunit of the protein kinase A as a cause of adrenal Cushing's syndrome: a European multicentric study.J Clin Endocrinol Metab. 2014 Oct;99(10):E2093-100. doi: 10.1210/jc.2014-2152. Epub 2014 Jul 24. J Clin Endocrinol Metab. 2014. PMID: 25057884
-
Protein kinase A defects and cortisol-producing adrenal tumors.Curr Opin Endocrinol Diabetes Obes. 2015 Jun;22(3):157-62. doi: 10.1097/MED.0000000000000149. Curr Opin Endocrinol Diabetes Obes. 2015. PMID: 25871963 Free PMC article. Review.
-
PRKACA: the catalytic subunit of protein kinase A and adrenocortical tumors.Front Cell Dev Biol. 2015 May 20;3:26. doi: 10.3389/fcell.2015.00026. eCollection 2015. Front Cell Dev Biol. 2015. PMID: 26042218 Free PMC article. Review.
Cited by
-
The cAMP-signaling cancers: Clinically-divergent disorders with a common central pathway.Front Endocrinol (Lausanne). 2022 Oct 13;13:1024423. doi: 10.3389/fendo.2022.1024423. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36313756 Free PMC article. Review.
-
Systematic identification of signal integration by protein kinase A.Proc Natl Acad Sci U S A. 2015 Apr 7;112(14):4501-6. doi: 10.1073/pnas.1409938112. Epub 2015 Mar 23. Proc Natl Acad Sci U S A. 2015. PMID: 25831502 Free PMC article.
-
Molecular Basis for Ser/Thr Specificity in PKA Signaling.Cells. 2020 Jun 25;9(6):1548. doi: 10.3390/cells9061548. Cells. 2020. PMID: 32630525 Free PMC article.
-
Spontaneous resolution of avascular necrosis of femoral heads following cure of Cushing's syndrome.Endocrinol Diabetes Metab Case Rep. 2016;2016:160015. doi: 10.1530/EDM-16-0015. Epub 2016 May 1. Endocrinol Diabetes Metab Case Rep. 2016. PMID: 27252864 Free PMC article.
-
Identification of a novel mutation of the PRKAR1A gene in a patient with Carney complex with significant osteoporosis and recurrent fractures.Hormones (Athens). 2016 Jan-Mar;15(1):129-35. doi: 10.14310/horm.2002.1627. Hormones (Athens). 2016. PMID: 27377598 Free PMC article. Review.
References
-
- Lindholm J, Juul S, Jørgensen JO, et al. Incidence and late prognosis of Cushing’s syndrome: a population-based study. J Clin Endocrinol Metab. 2001;86:117–23. - PubMed
-
- Newell-Price J, Bertagna X, Grossman AB, Nieman LK. Cushing’s syndrome. Lancet. 2006;367:1605–17. - PubMed
-
- Grumbach MM, Biller BM, Braunstein GD, et al. Management of the clinically inapparent adrenal mass (“incidentaloma”) Ann Intern Med. 2003;138:424–9. - PubMed
-
- Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev. 2004;25:309–40. - PubMed
-
- Terzolo M, Pia A, Reimondo G. Subclinical Cushing’s syndrome: definition and management. Clin Endocrinol (Oxf) 2012;76:12–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous