

Recombinant adenovirus type 5 HIV gag/pol/nef vaccine in South Africa: unblinded, long-term follow-up of the phase 2b HVTN 503/Phambili study
- PMID: 24560541
- PMCID: PMC4174314
- DOI: 10.1016/S1473-3099(14)70020-9
Recombinant adenovirus type 5 HIV gag/pol/nef vaccine in South Africa: unblinded, long-term follow-up of the phase 2b HVTN 503/Phambili study
Abstract
Background: The HVTN 503/Phambili study, which assessed the efficacy of the Merck Ad5 gag/pol/nef subtype B HIV-1 preventive vaccine in South Africa, was stopped when futility criteria in the Step study (assessing the same vaccine in the Americas, Caribbean, and Australia) were met. Here we report long-term follow-up data.
Methods: HVTN 503/Phambili was a double-blind, placebo-controlled, randomised trial that recruited HIV-1 uninfected, sexually active adults aged 18-35 years from five sites in South Africa. Eligible participants were randomly assigned (1:1) by computer-generated random numbers to either vaccine or placebo, stratified by site and sex. Cox proportional hazards models were used to estimate HIV-1 infection in the modified intention-to-treat cohort, all of whom were unmasked early in follow-up. The trial is registered with ClinicalTrials.gov, number NCT00413725 and the South African National Health Research Database, number DOH-27-0207-1539.
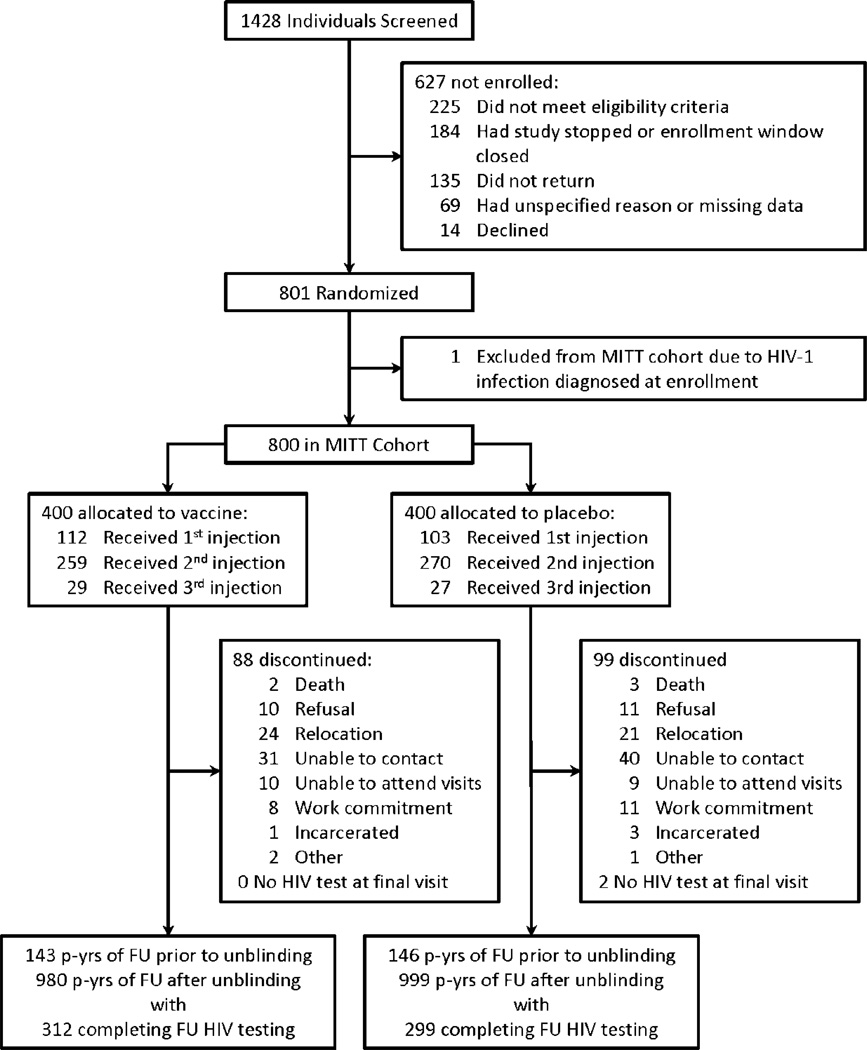
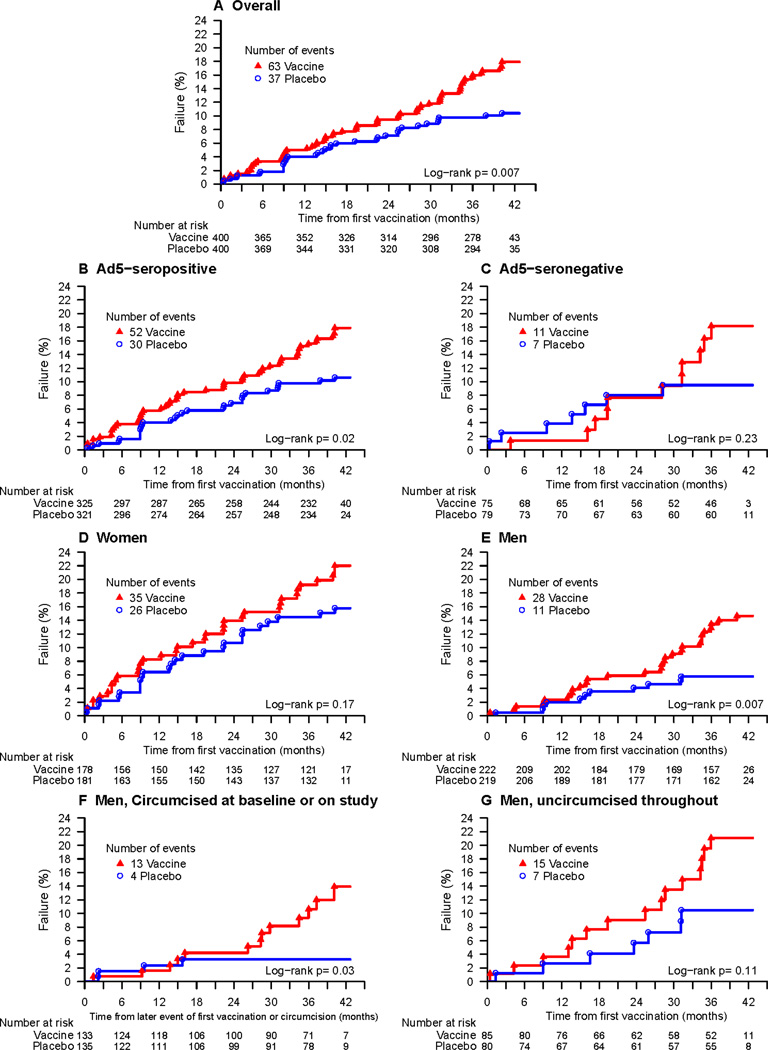
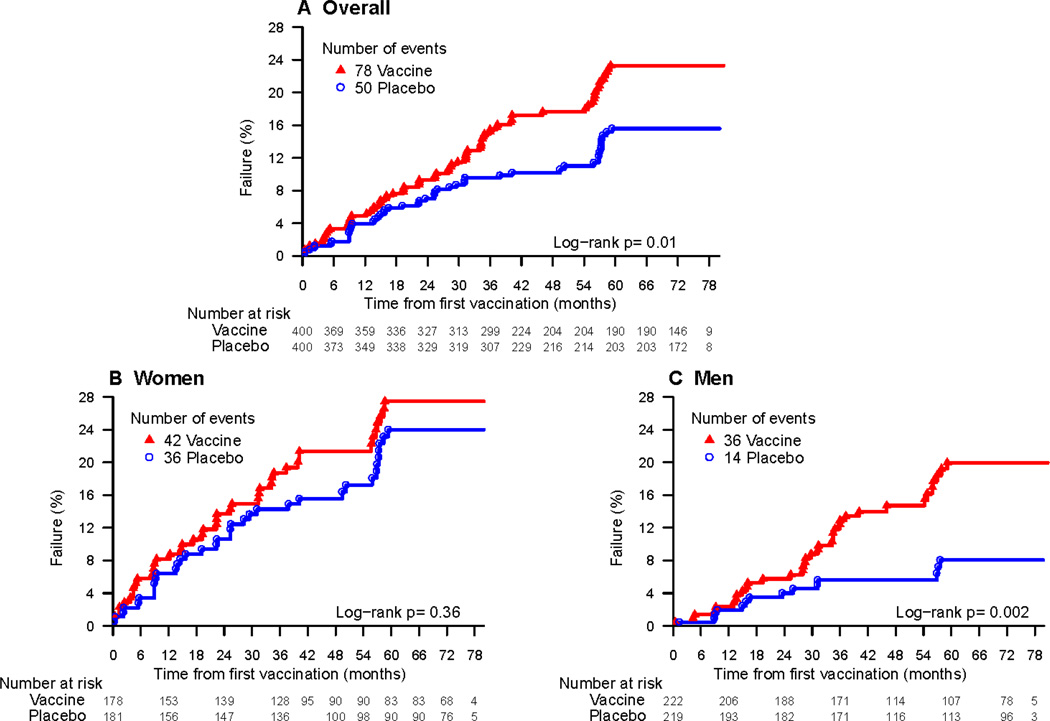
Findings: Between Jan 24, 2007, and Sept 19, 2007, 801 participants (26·7%) of a planned 3000 were randomly assigned (400 to vaccine, 401 to placebo); 216 (27%) received only one injection, 529 (66%) received only two injections, and 56 (7%) received three injections. At a median follow-up of 42 months (IQR 31-42), 63 vaccine recipients (16%) had HIV-1 infection compared with 37 placebo recipients (9%; adjusted HR 1·70, 95% CI 1·13-2·55; p=0·01). Risk for HIV-1 infection did not differ according to the number of vaccinations received, sex, circumcision, or adenovirus type 5 (Ad5) serostatus. Differences in risk behaviour at baseline or during the study, or annualised dropout rate (7·7% [95% CI 6·2-9·5] for vaccine recipients vs 8·8% [7·1-10·7] for placebo recipients; p=0·40) are unlikely explanations for the increased rate of HIV-1 infections seen in vaccine recipients.
Interpretation: The increased risk of HIV-1 acquisition in vaccine recipients, irrespective of number of doses received, warrants further investigation to understand the biological mechanism. We caution against further use of the Ad5 vector for HIV vaccines.
Funding: National Institute of Allergy and Infectious Diseases, Merck, and South African Medical Research Council.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Phambili: moving forward without the blindfold.Lancet Infect Dis. 2014 May;14(5):361-2. doi: 10.1016/S1473-3099(14)70029-5. Epub 2014 Feb 20. Lancet Infect Dis. 2014. PMID: 24560542 No abstract available.
Similar articles
-
Safety and efficacy of the HVTN 503/Phambili study of a clade-B-based HIV-1 vaccine in South Africa: a double-blind, randomised, placebo-controlled test-of-concept phase 2b study.Lancet Infect Dis. 2011 Jul;11(7):507-15. doi: 10.1016/S1473-3099(11)70098-6. Epub 2011 May 11. Lancet Infect Dis. 2011. PMID: 21570355 Free PMC article. Clinical Trial.
-
Continued Follow-Up of Phambili Phase 2b Randomized HIV-1 Vaccine Trial Participants Supports Increased HIV-1 Acquisition among Vaccinated Men.PLoS One. 2015 Sep 14;10(9):e0137666. doi: 10.1371/journal.pone.0137666. eCollection 2015. PLoS One. 2015. PMID: 26368824 Free PMC article. Clinical Trial.
-
A study of vaccine-induced immune pressure on breakthrough infections in the Phambili phase 2b HIV-1 vaccine efficacy trial.Vaccine. 2016 Nov 11;34(47):5792-5801. doi: 10.1016/j.vaccine.2016.09.054. Epub 2016 Oct 15. Vaccine. 2016. PMID: 27756485 Free PMC article. Clinical Trial.
-
Overview of STEP and Phambili trial results: two phase IIb test-of-concept studies investigating the efficacy of MRK adenovirus type 5 gag/pol/nef subtype B HIV vaccine.Curr Opin HIV AIDS. 2010 Sep;5(5):357-61. doi: 10.1097/COH.0b013e32833d2d2b. Curr Opin HIV AIDS. 2010. PMID: 20978374 Free PMC article. Review.
-
Nonreplicating vectors in HIV vaccines.Curr Opin HIV AIDS. 2013 Sep;8(5):412-20. doi: 10.1097/COH.0b013e328363d3b7. Curr Opin HIV AIDS. 2013. PMID: 23925001 Free PMC article. Review.
Cited by
-
Live attenuated varicella-zoster virus vaccine does not induce HIV target cell activation.J Clin Invest. 2019 Feb 1;129(2):875-886. doi: 10.1172/JCI124473. Epub 2019 Jan 22. J Clin Invest. 2019. PMID: 30511963 Free PMC article. Clinical Trial.
-
FcγR Genetic Variation and HIV-1 Vaccine Efficacy: Context And Considerations.Front Immunol. 2021 Dec 15;12:788203. doi: 10.3389/fimmu.2021.788203. eCollection 2021. Front Immunol. 2021. PMID: 34975881 Free PMC article.
-
Challenges in HIV Vaccine Research for Treatment and Prevention.Front Immunol. 2014 Sep 8;5:417. doi: 10.3389/fimmu.2014.00417. eCollection 2014. Front Immunol. 2014. PMID: 25250026 Free PMC article. Review.
-
Predicting Overall Vaccine Efficacy in a New Setting by Re-Calibrating Baseline Covariate and Intermediate Response Endpoint Effect Modifiers of Type-Specific Vaccine Efficacy.Epidemiol Methods. 2016 Dec;5(1):93-112. doi: 10.1515/em-2015-0007. Epub 2016 Jan 23. Epidemiol Methods. 2016. PMID: 28154793 Free PMC article.
-
Promise and problems associated with the use of recombinant AAV for the delivery of anti-HIV antibodies.Mol Ther Methods Clin Dev. 2016 Nov 16;3:16068. doi: 10.1038/mtm.2016.68. eCollection 2016. Mol Ther Methods Clin Dev. 2016. PMID: 28197421 Free PMC article. Review.
References
-
- Sheets RL, Stein J, Bailer RT, et al. Biodistribution and toxicological safety of adenovirus type 5 and type 35 vectored vaccines against human immunodeficiency virus-1 (HIV-1), Ebola, or Marburg are similar despite differing adenovirus serotype vector, manufacturer's construct, or gene inserts. J Immunotoxicol. 2008 Jul;5(3):315–335. PubMed PMID: 18830892; PubMed Central PMCID: PMC2777703. - PMC - PubMed
-
- Liu J, Ewald BA, Lynch DM, et al. Magnitude and phenotype of cellular immune responses elicited by recombinant adenovirus vectors and heterologous prime-boost regimens in rhesus monkeys. J Virol. 2008 May;82(10):4844–4852. Epub 2008 Mar 12. PubMed PMID: 18337575; PubMed Central PMCID: PMC2346755. - PMC - PubMed
-
- Barratt-Boyes SM, Soloff AC, Gao W, et al. Broad cellular immunity with robust memory responses to simian immunodeficiency virus following serial vaccination with adenovirus 5- and 35-based vectors. J Gen Virol. 2006 Jan;87(Pt 1):139–149. PubMed PMID: 16361426. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1 AI069519/AI/NIAID NIH HHS/United States
- 5U01 AI068614/AI/NIAID NIH HHS/United States
- U01 AI069453/AI/NIAID NIH HHS/United States
- 5U01 AI069469/AI/NIAID NIH HHS/United States
- UM1 AI069469/AI/NIAID NIH HHS/United States
- UM1 AI068614/AI/NIAID NIH HHS/United States
- UM1 AI069453/AI/NIAID NIH HHS/United States
- 5U01 AI069453/AI/NIAID NIH HHS/United States
- U01 AI069519/AI/NIAID NIH HHS/United States
- U01 AI068618/AI/NIAID NIH HHS/United States
- 5U01 AI068635/AI/NIAID NIH HHS/United States
- U01 AI068614/AI/NIAID NIH HHS/United States
- UM1 AI068618/AI/NIAID NIH HHS/United States
- 5U01 AI068618/AI/NIAID NIH HHS/United States
- U01 AI069469/AI/NIAID NIH HHS/United States
- U01 AI068635/AI/NIAID NIH HHS/United States
- UM1 AI068635/AI/NIAID NIH HHS/United States
- 5U01 AI069519/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
