

Traumatic Brain Injury pathophysiology and treatments: early, intermediate, and late phases post-injury
- PMID: 24381049
- PMCID: PMC3907812
- DOI: 10.3390/ijms15010309
Traumatic Brain Injury pathophysiology and treatments: early, intermediate, and late phases post-injury
Abstract
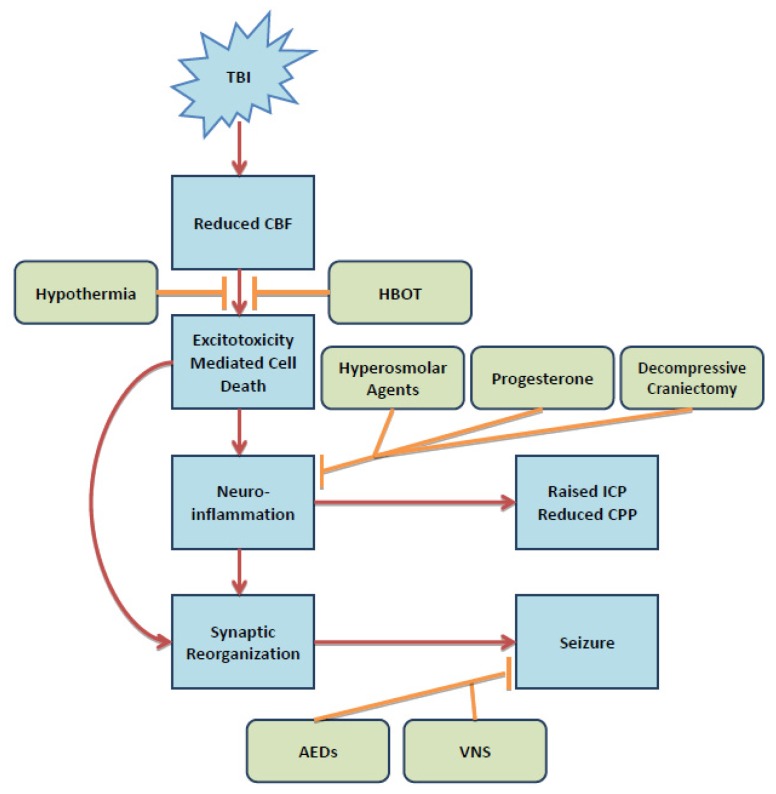
Traumatic Brain Injury (TBI) affects a large proportion and extensive array of individuals in the population. While precise pathological mechanisms are lacking, the growing base of knowledge concerning TBI has put increased emphasis on its understanding and treatment. Most treatments of TBI are aimed at ameliorating secondary insults arising from the injury; these insults can be characterized with respect to time post-injury, including early, intermediate, and late pathological changes. Early pathological responses are due to energy depletion and cell death secondary to excitotoxicity, the intermediate phase is characterized by neuroinflammation and the late stage by increased susceptibility to seizures and epilepsy. Current treatments of TBI have been tailored to these distinct pathological stages with some overlap. Many prophylactic, pharmacologic, and surgical treatments are used post-TBI to halt the progression of these pathologic reactions. In the present review, we discuss the mechanisms of the pathological hallmarks of TBI and both current and novel treatments which target the respective pathways.
Figures
Similar articles
-
Cooling the injured brain: how does moderate hypothermia influence the pathophysiology of traumatic brain injury.Curr Pharm Des. 2007;13(22):2310-22. doi: 10.2174/138161207781368756. Curr Pharm Des. 2007. PMID: 17692002 Review.
-
Antiepileptics for Post-Traumatic Seizure Prophylaxis after Traumatic Brain Injury.Curr Pharm Des. 2017;23(42):6428-6441. doi: 10.2174/1381612823666171031100139. Curr Pharm Des. 2017. PMID: 29086674 Review.
-
Long-lasting blood-brain barrier dysfunction and neuroinflammation after traumatic brain injury.Neurobiol Dis. 2020 Nov;145:105080. doi: 10.1016/j.nbd.2020.105080. Epub 2020 Sep 9. Neurobiol Dis. 2020. PMID: 32919030
-
Anti-epileptogenesis in rodent post-traumatic epilepsy models.Neurosci Lett. 2011 Jun 27;497(3):163-71. doi: 10.1016/j.neulet.2011.02.033. Epub 2011 Mar 21. Neurosci Lett. 2011. PMID: 21402123 Review.
-
From traumatic brain injury to posttraumatic epilepsy: what animal models tell us about the process and treatment options.Epilepsia. 2009 Feb;50 Suppl 2:21-9. doi: 10.1111/j.1528-1167.2008.02007.x. Epilepsia. 2009. PMID: 19187291 Review.
Cited by
-
Monotrauma is associated with enhanced remote inflammatory response and organ damage, while polytrauma intensifies both in porcine trauma model.Eur J Trauma Emerg Surg. 2020 Feb;46(1):31-42. doi: 10.1007/s00068-019-01098-1. Epub 2019 Mar 12. Eur J Trauma Emerg Surg. 2020. PMID: 30864051
-
Incidence and risk factors associated with pressure injury in patients with traumatic brain injury.Int J Nurs Pract. 2020 Jun;26(3):e12821. doi: 10.1111/ijn.12821. Epub 2020 Jan 29. Int J Nurs Pract. 2020. PMID: 31994827 Free PMC article.
-
Breaking barriers in trauma research: A narrative review of opportunities to leverage veterinary trauma for accelerated translation to clinical solutions for pets and people.J Clin Transl Sci. 2024 Apr 5;8(1):e74. doi: 10.1017/cts.2024.513. eCollection 2024. J Clin Transl Sci. 2024. PMID: 38715566 Free PMC article. Review.
-
Scaffolding protein Homer1a protects against NMDA-induced neuronal injury.Cell Death Dis. 2015 Aug 6;6(8):e1843. doi: 10.1038/cddis.2015.216. Cell Death Dis. 2015. PMID: 26247728 Free PMC article.
-
Mitophagy and Traumatic Brain Injury: Regulatory Mechanisms and Therapeutic Potentials.Oxid Med Cell Longev. 2023 Feb 17;2023:1649842. doi: 10.1155/2023/1649842. eCollection 2023. Oxid Med Cell Longev. 2023. PMID: 36846712 Free PMC article. Review.
References
-
- Faul M.X.L., Wald M.M., Coronado V.G. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations, and Deaths. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; Atlanta, GA, USA: 2010.
-
- Lu J., Marmarou A., Choi S., Maas A., Murray G., Steyerberg E.W. Mortality from traumatic brain injury. Acta Neurochir. Suppl. 2005;95:281–285. - PubMed
-
- Ghajar J., Hariri R.J., Narayan R.K., Iacono L.A., Firlik K., Patterson R.H. Survey of critical care management of comatose, head-injured patients in the United States. Crit. Care Med. 1995;23:560–567. - PubMed
-
- Hesdorffer D.C., Ghajar J., Iacono L. Predictors of compliance with the evidence-based guidelines for traumatic brain injury care: A survey of United States trauma centers. J. Trauma. 2002;52:1202–1209. - PubMed
-
- Leung L.Y., Wei G., Shear D.A., Tortella F.C. The acute effects of hemorrhagic shock on cerebral blood flow, brain tissue oxygen tension, and spreading depolarization following penetrating ballistic-like brain injury. J. Neurotrauma. 2013;30:1288–1298. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
