

Amifostine protects vascularity and improves union in a model of irradiated mandibular fracture healing
- PMID: 24281582
- PMCID: PMC3857216
- DOI: 10.1097/PRS.0b013e3182a80766
Amifostine protects vascularity and improves union in a model of irradiated mandibular fracture healing
Abstract
Background: Pathologic fractures of the mandible can be devastating to cancer patients and are due in large part to the pernicious effects of irradiation on bone vascularity. The authors' aim was to ascertain whether amifostine, a radioprotective drug, will preserve vascularity and improve bone healing in a murine model of irradiated mandibular fracture repair.
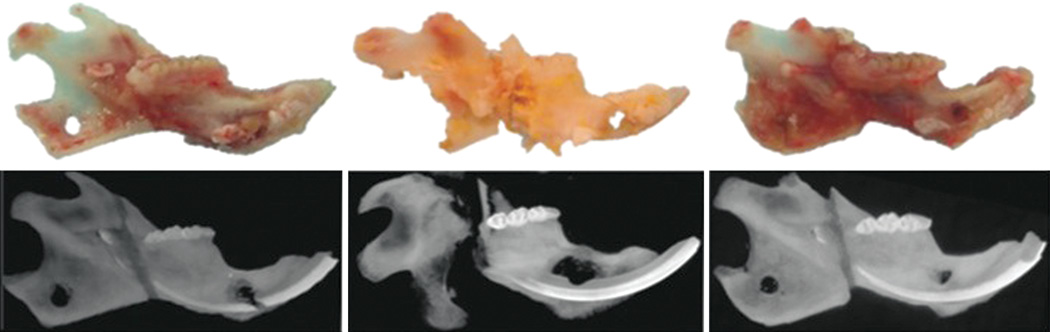
Methods: Rats were randomized into three groups: nonirradiated fracture (n = 9), irradiation/fracture (n = 5), and amifostine/irradiation/fracture (n = 7). Animals in the irradiation groups underwent a human equivalent dose of radiation directed at the left hemimandible. Animals treated in the amifostine group received amifostine concomitantly with radiation. All animals underwent unilateral left mandibular osteotomy with external fixation set to a 2.1-mm fracture gap. Fracture healing was allowed for 40 days before perfusion with Microfil. Vascular radiomorphometrics were quantified with micro-computed tomography.
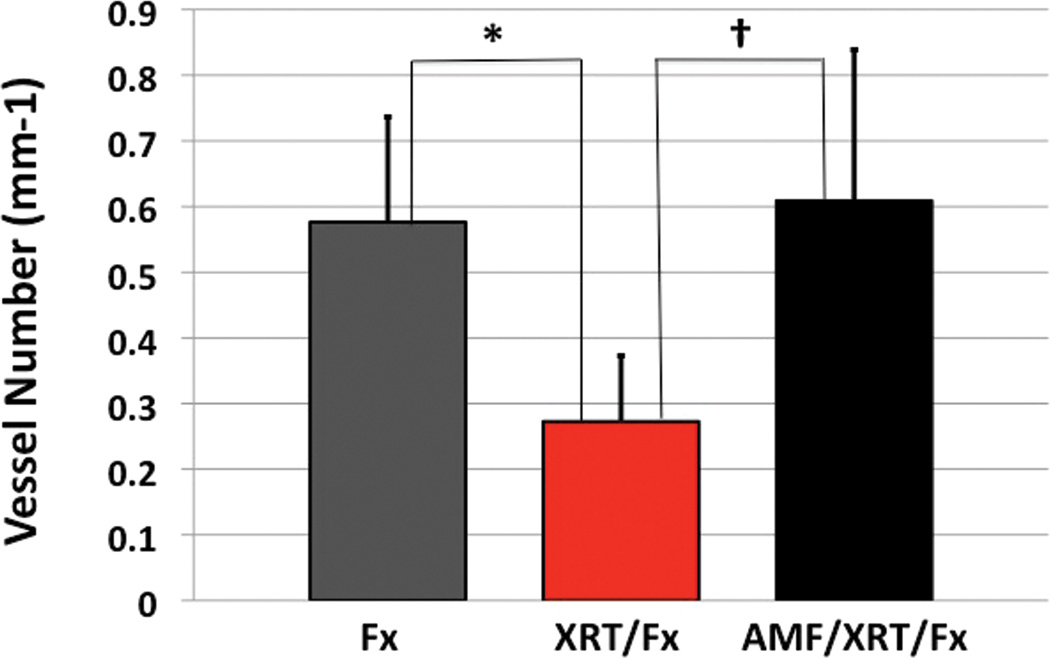
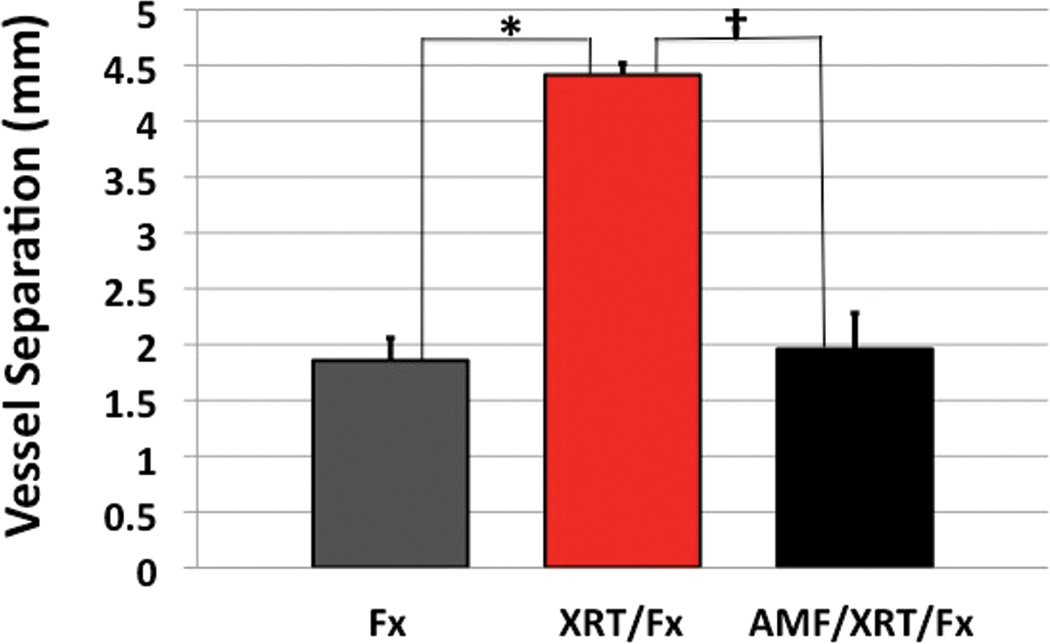
Results: When compared with the irradiated/fractured group, amifostine treatment more than doubled the rate of fracture unions to 57 percent. Amifostine treatment also resulted in an increase in vessel number (123 percent; p < 0.05) and a corresponding decrease in vessel separation (55.5 percent; p < 0.05) there was no statistical difference in the vascularity metrics between the amifostine/irradiation/fracture group and the nonirradiated/fracture group.
Conclusions: Amifostine prophylaxis during radiation maintains mandibular vascularity at levels observed in nonirradiated fracture specimens, corresponding to improved unions. These results set the stage for clinical exploration of this targeted therapy alone and in combination with other treatments, to mitigate the effects of irradiation on bone healing and fracture repair.
Figures

Similar articles
-
Deferoxamine restores callus size, mineralization, and mechanical strength in fracture healing after radiotherapy.Plast Reconstr Surg. 2013 May;131(5):711e-719e. doi: 10.1097/PRS.0b013e3182865c57. Plast Reconstr Surg. 2013. PMID: 23629110 Free PMC article.
-
Microdensitometric and microarchitectural alterations in irradiated mandibular fracture repair.J Craniofac Surg. 2014 Nov;25(6):2022-6. doi: 10.1097/SCS.0000000000000520. J Craniofac Surg. 2014. PMID: 25304138
-
Quantitative histologic evidence of amifostine-induced cytoprotection in an irradiated murine model of mandibular distraction osteogenesis.Plast Reconstr Surg. 2012 Dec;130(6):1199-1207. doi: 10.1097/PRS.0b013e31826d2201. Plast Reconstr Surg. 2012. PMID: 22878481 Free PMC article.
-
Prevention of radiation-induced central nervous system toxicity: a role for amifostine?Anticancer Res. 2004 Nov-Dec;24(6):3803-9. Anticancer Res. 2004. PMID: 15736415 Review.
-
Protection of normal tissues from the cytotoxic effects of chemotherapy and radiation by amifostine (WR-2721): preclinical aspects.Eur J Cancer. 1995;31A Suppl 1:S1-7. doi: 10.1016/0959-8049(95)00145-9. Eur J Cancer. 1995. PMID: 7577093 Review.
Cited by
-
Protective Effect and Mechanism of Action of Rosmarinic Acid on Radiation-Induced Parotid Gland Injury in Rats.Dose Response. 2020 Feb 20;18(1):1559325820907782. doi: 10.1177/1559325820907782. eCollection 2020 Jan-Mar. Dose Response. 2020. PMID: 32127788 Free PMC article.
-
Amifostine and Melatonin Prevent Acute Salivary Gland Dysfunction 10 Days After Radiation Through Anti-Ferroptosis and Anti-Ferritinophagy Effects.Int J Mol Sci. 2024 Oct 29;25(21):11613. doi: 10.3390/ijms252111613. Int J Mol Sci. 2024. PMID: 39519165 Free PMC article.
-
Vascular Remodelling Relates to an Elevated Oscillatory Shear Index and Relative Residence Time in Spontaneously Hypertensive Rats.Sci Rep. 2017 May 17;7(1):2007. doi: 10.1038/s41598-017-01906-x. Sci Rep. 2017. PMID: 28515420 Free PMC article.
-
Pharmacological interventions for the prevention of insufficiency fractures and avascular necrosis associated with pelvic radiotherapy in adults.Cochrane Database Syst Rev. 2018 Apr 23;4(4):CD010604. doi: 10.1002/14651858.CD010604.pub2. Cochrane Database Syst Rev. 2018. PMID: 29683475 Free PMC article. Review.
-
Novel Formulation Strategy to Improve the Feasibility of Amifostine Administration.Pharm Res. 2018 Mar 19;35(5):99. doi: 10.1007/s11095-018-2386-5. Pharm Res. 2018. PMID: 29556791
References
-
- Bourhis J, Overgaard J, Audry H, et al. Hyperfractionated or accelerated radiotherapy in head and neck cancer: a meta-analysis. Lancet. 2006;368(9538):843–854. - PubMed
-
- Bonarigo BC, Rubin P. Nonunion of pathologic fracture after radiation therapy. Radiology. 1967;88:889–898. - PubMed
-
- Ezsias A, Sugar W. Pathological Fractures of the Mandible: A Diagnostic and Treatment Dilemma. Br J Oral Maxillofac Surg. 1994;32:303–306. - PubMed
-
- Gerhards F, Kuffner HD, Wagner W. Pathological fractures of the mandible: A review of the etiology and treatment. Int J Oral Maxillofac Surg. 1998;27:186–190. - PubMed
-
- Moulton-Barret R, Rubinstein AJ, Salzhauer MA, et al. Complications of mandibular fractures. Ann Plast Surg. 1998;41:258–263. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
