

Cabozantinib inhibits prostate cancer growth and prevents tumor-induced bone lesions
- PMID: 24097861
- PMCID: PMC3946460
- DOI: 10.1158/1078-0432.CCR-13-0839
Cabozantinib inhibits prostate cancer growth and prevents tumor-induced bone lesions
Abstract
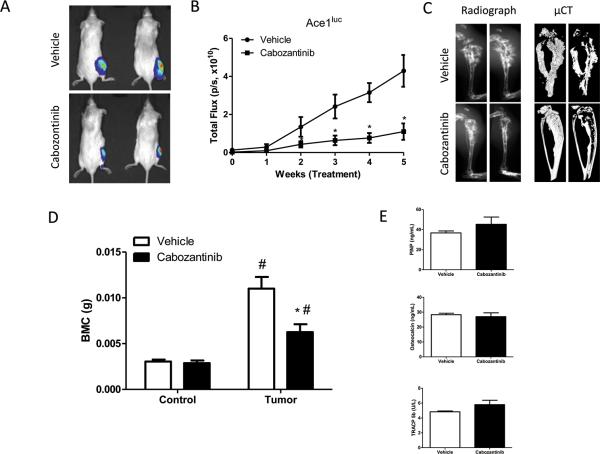
Purpose: Cabozantinib, an orally available multityrosine kinase inhibitor with activity against mesenchymal epithelial transition factor (MET) and VEGF receptor 2 (VEGFR2), induces resolution of bone scan lesions in men with castration-resistant prostate cancer bone metastases. The purpose of this study was to determine whether cabozantinib elicited a direct antitumor effect, an indirect effect through modulating bone, or both.
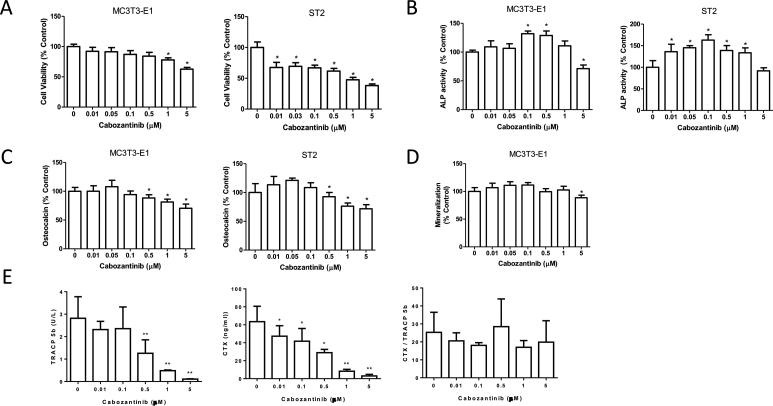
Experimental design: Using human prostate cancer xenograft studies in mice, we determined the impact of cabozantinib on tumor growth in soft tissue and bone. In vitro studies with cabozantinib were performed using (i) prostate cancer cell lines to evaluate its impact on cell growth, invasive ability, and MET and (ii) osteoblast cell lines to evaluate its impact on viability and differentiation and VEGFR2.
Results: Cabozantinib inhibited progression of multiple prostate cancer cell lines (Ace-1, C4-2B, and LuCaP 35) in bone metastatic and soft tissue murine models of prostate cancer, except for PC-3 prostate cancer cells in which it inhibited only subcutaneous growth. Cabozantinib directly inhibited prostate cancer cell viability and induced apoptosis in vitro and in vivo and inhibited cell invasion in vitro. Cabozantinib had a dose-dependent biphasic effect on osteoblast activity and inhibitory effect on osteoclast production in vitro that was reflected in vivo. It blocked MET and VEGFR2 phosphorylation in prostate cancer cells and osteoblast-like cells, respectively.
Conclusion: These data indicate that cabozantinib has direct antitumor activity, and that its ability to modulate osteoblast activity may contribute to its antitumor efficacy.
©2013 AACR.
Figures




Comment in
-
Cabozantinib and prostate cancer: inhibiting seed and disrupting soil?Clin Cancer Res. 2014 Feb 1;20(3):525-7. doi: 10.1158/1078-0432.CCR-13-2636. Epub 2013 Nov 27. Clin Cancer Res. 2014. PMID: 24284057 Free PMC article.
Similar articles
-
Dual targeting c-met and VEGFR2 in osteoblasts suppresses growth and osteolysis of prostate cancer bone metastasis.Cancer Lett. 2018 Feb 1;414:205-213. doi: 10.1016/j.canlet.2017.11.016. Epub 2017 Nov 22. Cancer Lett. 2018. PMID: 29174801
-
Cabozantinib inhibits growth of androgen-sensitive and castration-resistant prostate cancer and affects bone remodeling.PLoS One. 2013 Oct 25;8(10):e78881. doi: 10.1371/journal.pone.0078881. eCollection 2013. PLoS One. 2013. PMID: 24205338 Free PMC article.
-
Integrating Murine and Clinical Trials with Cabozantinib to Understand Roles of MET and VEGFR2 as Targets for Growth Inhibition of Prostate Cancer.Clin Cancer Res. 2016 Jan 1;22(1):107-21. doi: 10.1158/1078-0432.CCR-15-0235. Epub 2015 Aug 13. Clin Cancer Res. 2016. PMID: 26272062 Free PMC article.
-
Current role of cabozantinib in metastatic castration-resistant prostate cancer.Expert Rev Anticancer Ther. 2015 Feb;15(2):151-6. doi: 10.1586/14737140.2015.1003047. Epub 2015 Jan 14. Expert Rev Anticancer Ther. 2015. PMID: 25586337 Review.
-
Cabozantinib: a MET, RET, and VEGFR2 tyrosine kinase inhibitor.Recent Results Cancer Res. 2014;201:207-14. doi: 10.1007/978-3-642-54490-3_12. Recent Results Cancer Res. 2014. PMID: 24756794 Review.
Cited by
-
(18)F-FDG-PET/CT and (18)F-NaF-PET/CT in men with castrate-resistant prostate cancer.Am J Nucl Med Mol Imaging. 2014 Dec 15;5(1):72-82. eCollection 2015. Am J Nucl Med Mol Imaging. 2014. PMID: 25625029 Free PMC article.
-
GDF15 promotes prostate cancer bone metastasis and colonization through osteoblastic CCL2 and RANKL activation.Bone Res. 2022 Jan 20;10(1):6. doi: 10.1038/s41413-021-00178-6. Bone Res. 2022. PMID: 35058441 Free PMC article.
-
A phase I study of cabozantinib (XL184) in patients with renal cell cancer.Ann Oncol. 2014 Aug;25(8):1603-8. doi: 10.1093/annonc/mdu184. Epub 2014 May 14. Ann Oncol. 2014. PMID: 24827131 Free PMC article. Clinical Trial.
-
Non-genotoxic conditioning for hematopoietic stem cell transplantation using a hematopoietic-cell-specific internalizing immunotoxin.Nat Biotechnol. 2016 Jul;34(7):738-45. doi: 10.1038/nbt.3584. Epub 2016 Jun 6. Nat Biotechnol. 2016. PMID: 27272386 Free PMC article.
-
Cabozantinib (XL184) and R428 (BGB324) Inhibit the Growth of Esophageal Squamous Cell Carcinoma (ESCC).Front Oncol. 2019 Nov 6;9:1138. doi: 10.3389/fonc.2019.01138. eCollection 2019. Front Oncol. 2019. PMID: 31781483 Free PMC article.
References
-
- Shah RB, Mehra R, Chinnaiyan AM, Shen R, Ghosh D, Zhou M, et al. Androgen-independent prostate cancer is a heterogeneous group of diseases: lessons from a rapid autopsy program. Cancer Res. 2004;64:9209–16. - PubMed
-
- Dy SM, Asch SM, Naeim A, Sanati H, Walling A, Lorenz KA. Evidence-based standards for cancer pain management. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2008;26:3879–85. - PubMed
-
- Mercadante S, Fulfaro F. Management of painful bone metastases. Curr Opin Oncol. 2007;19:308–14. - PubMed
-
- Rajpar S, Fizazi K. Bone targeted therapies in metastatic castration-resistant prostate cancer. Cancer J. 2013;19:66–70. - PubMed
-
- Stella GM, Benvenuti S, Comoglio PM. Targeting the MET oncogene in cancer and metastases. Expert opinion on investigational drugs. 2010;19:1381–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
