

Periosteum: biology and applications in craniofacial bone regeneration
- PMID: 24088412
- PMCID: PMC3895334
- DOI: 10.1177/0022034513506445
Periosteum: biology and applications in craniofacial bone regeneration
Abstract
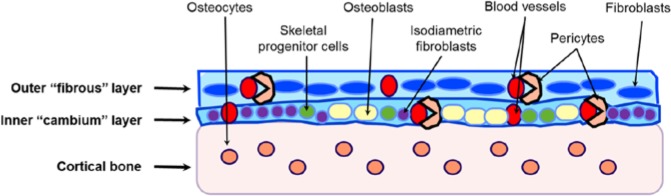
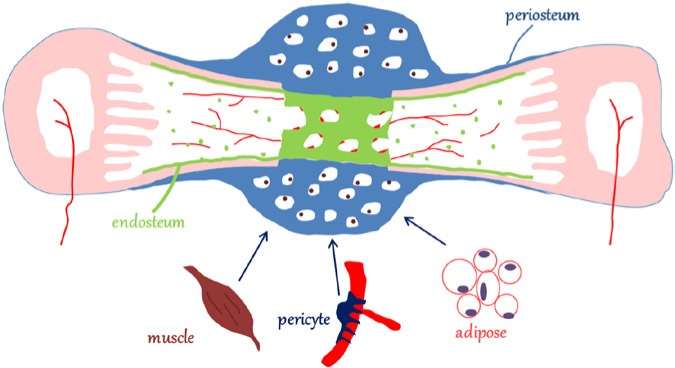
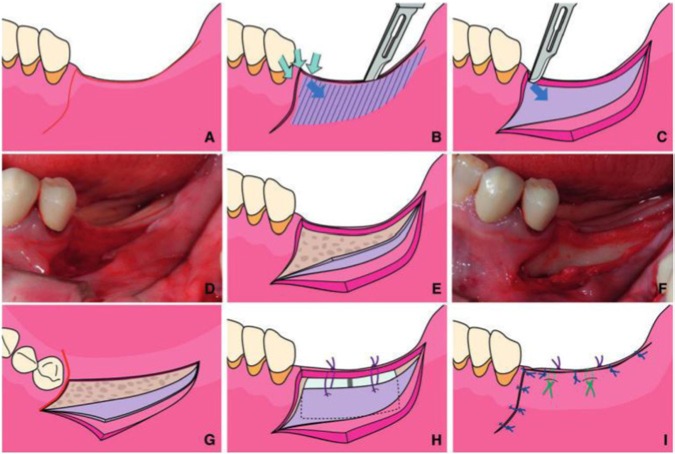
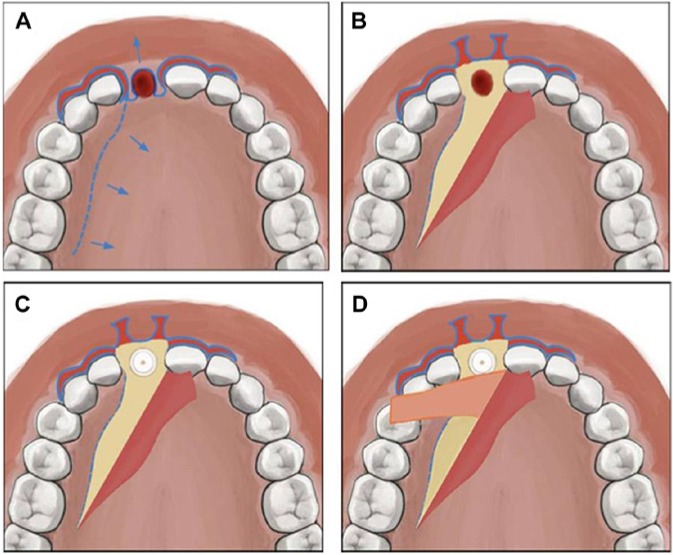
The bone-regenerative potentials of the periosteum have been explored as early as the 17th century. Over the past few years, however, much has been discovered in terms of the molecular and cellular mechanisms that control the periosteal contribution to bone regeneration. Lineage tracing analyses and knock-in transgenic mice have helped define the relative contributions of the periosteum and endosteum to bone regeneration. Additional studies have shed light on the critical roles that BMP, FGF, Hedgehog, Notch, PDGF, Wnt, and inflammation signaling have or may have in periosteal-mediated bone regeneration, fostering the path to novel approaches in bone-regenerative therapy. Thus, by examining the role that each pathway has in periosteal-mediated bone regeneration, in this review we analyze the status of the current research on the regenerative potential of the periosteum. The provided analysis aims to inform both clinician-scientists who may have interest in the current studies about the biology of the periosteum as well as dental surgeons who may find this review useful to perform periosteal-harnessing bone-regenerative procedures.
Keywords: bone healing; osteoprogenitor cells; periosteum; regenerative surgery; stem cells; tissue engineering.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Figures

Similar articles
-
Current insights on the regenerative potential of the periosteum: molecular, cellular, and endogenous engineering approaches.J Orthop Res. 2012 Dec;30(12):1869-78. doi: 10.1002/jor.22181. Epub 2012 Jul 9. J Orthop Res. 2012. PMID: 22778049 Free PMC article. Review.
-
Translating Periosteum's Regenerative Power: Insights From Quantitative Analysis of Tissue Genesis With a Periosteum Substitute Implant.Stem Cells Transl Med. 2016 Dec;5(12):1739-1749. doi: 10.5966/sctm.2016-0004. Epub 2016 Jul 27. Stem Cells Transl Med. 2016. PMID: 27465072 Free PMC article.
-
The potential for vertical bone regeneration via maxillary periosteal elevation.J Clin Periodontol. 2014 Dec;41(12):1170-7. doi: 10.1111/jcpe.12310. Epub 2014 Nov 11. J Clin Periodontol. 2014. PMID: 25229322
-
Periosteal Skeletal Stem and Progenitor Cells in Bone Regeneration.Curr Osteoporos Rep. 2022 Oct;20(5):334-343. doi: 10.1007/s11914-022-00737-8. Epub 2022 Jul 13. Curr Osteoporos Rep. 2022. PMID: 35829950 Review.
-
Periosteum-derived Micrografts for bone regeneration.Connect Tissue Res. 2023 Jul;64(4):400-412. doi: 10.1080/03008207.2023.2206489. Epub 2023 May 17. Connect Tissue Res. 2023. PMID: 37195000
Cited by
-
Periosteum Containing Implicit Stem Cells: A Progressive Source of Inspiration for Bone Tissue Regeneration.Int J Mol Sci. 2024 Feb 10;25(4):2162. doi: 10.3390/ijms25042162. Int J Mol Sci. 2024. PMID: 38396834 Free PMC article. Review.
-
Lineage Differentiation Potential of Different Sources of Mesenchymal Stem Cells for Osteoarthritis Knee.Pharmaceuticals (Basel). 2022 Mar 22;15(4):386. doi: 10.3390/ph15040386. Pharmaceuticals (Basel). 2022. PMID: 35455383 Free PMC article. Review.
-
Characterization of the F-box Proteins FBXW2 and FBXL14 in the Initiation of Bone Regeneration in Transplants given to Nude Mice.Open Biomed Eng J. 2018 Oct 18;12:75-89. doi: 10.2174/1874120701812010075. eCollection 2018. Open Biomed Eng J. 2018. PMID: 30450135 Free PMC article.
-
HIF-1α Regulates Osteogenesis of Periosteum-Derived Stem Cells Under Hypoxia Conditions via Modulating POSTN Expression.Front Cell Dev Biol. 2022 Feb 17;10:836285. doi: 10.3389/fcell.2022.836285. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 35252198 Free PMC article.
-
Macrophage-lineage TRAP+ cells recruit periosteum-derived cells for periosteal osteogenesis and regeneration.J Clin Invest. 2019 Apr 4;129(6):2578-2594. doi: 10.1172/JCI98857. J Clin Invest. 2019. PMID: 30946695 Free PMC article.
References
-
- Abrahamsson P, Walivaara DA, Isaksson S, Andersson G. (2012). Periosteal expansion before local bone reconstruction using a new technique for measuring soft tissue profile stability: a clinical study. J Oral Maxillofac Surg 70:e521-e530. - PubMed
-
- Agholme F, Isaksson H, Kuhstoss S, Aspenberg P. (2011). The effects of Dickkopf-1 antibody on metaphyseal bone and implant fixation under different loading conditions. Bone 48:988-996. - PubMed
-
- Allen MR, Burr DB. (2005). Human femoral neck has less cellular periosteum, and more mineralized periosteum, than femoral diaphyseal bone. Bone 36:311-316. - PubMed
-
- Allen MR, Hock JM, Burr DB. (2004). Periosteum: biology, regulation, and response to osteoporosis therapies. Bone 35:1003-1012. - PubMed
-
- Blaisdell FE. (1925). The osteogenic function of periosteum. Arch Surg 11:933.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
