

Takayasu arteritis: criteria for surgical intervention should not be ignored
- PMID: 23986869
- PMCID: PMC3748735
- DOI: 10.1155/2013/618910
Takayasu arteritis: criteria for surgical intervention should not be ignored
Abstract
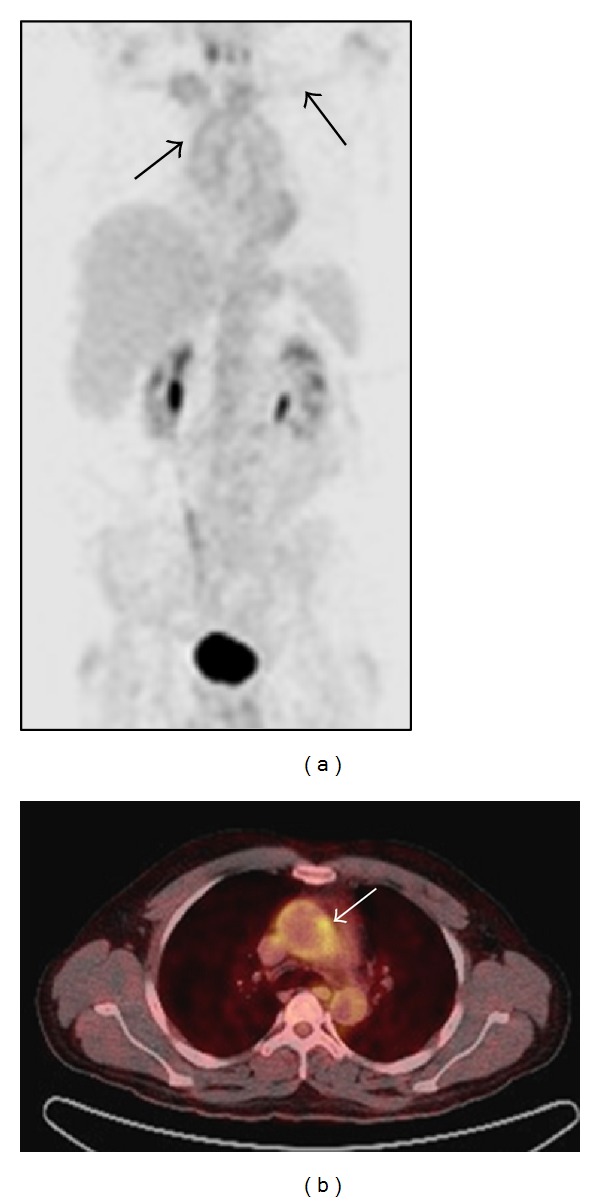
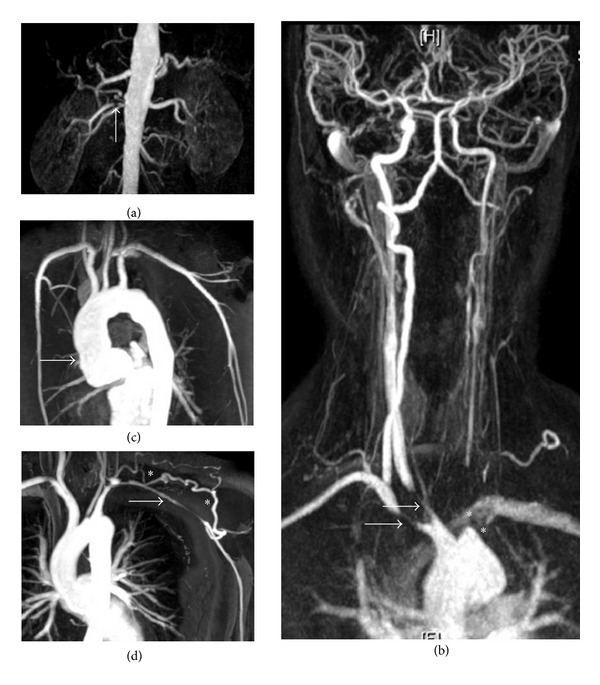
Takayasu aortoarteritis is a rare, chronic granulomatous panarteritis with significant morbidity amongst young patients. Current challenges include a lack of awareness about the condition, delays in diagnosis due to its varied presentation, and suboptimal methods for assessing disease activity. The development of noninvasive imaging including magnetic resonance angiography and positron emission tomography is aiding earlier diagnosis. Early initiation of immunosuppressive treatment is crucial to control active inflammation and minimize arterial injury. Recent studies investigating biological agents such as tumour necrosis factor- α antagonists are encouraging. Surgical revascularization should only be undertaken following careful consideration, as restenosis is common. The indications for considering intervention include uncontrolled hypertension due to renal artery stenosis, severe symptomatic coronary artery or cerebrovascular disease, severe aortic regurgitation, stenotic or occlusive lesions resulting in critical limb ischemia, and aneurysms at risk of rupture. In these cases, the risk benefit ratio for intervention is good. Open surgery, at present, has better outcomes compared to endovascular techniques. However, technological advances in endovascular treatment are continually improving. Controlling disease activity prior to and following revascularization is key to preventing complications. A multidisciplinary approach to the diagnosis and management of Takayasu arteritis is essential to achieve satisfactory patient outcomes.
Figures

Similar articles
-
Takayasu arteritis in paediatrics.Cardiol Young. 2018 Mar;28(3):354-361. doi: 10.1017/S1047951117001998. Epub 2017 Dec 13. Cardiol Young. 2018. PMID: 29233197 Review.
-
Regressed coronary ostial stenosis in a young female with Takayasu arteritis: a case report.BMC Cardiovasc Disord. 2019 Apr 2;19(1):79. doi: 10.1186/s12872-019-1066-7. BMC Cardiovasc Disord. 2019. PMID: 30940076 Free PMC article.
-
Endovascular revascularization for carotid artery occlusion in patients with Takayasu arteritis.Eur J Vasc Endovasc Surg. 2015 May;49(5):498-505. doi: 10.1016/j.ejvs.2015.01.018. Epub 2015 Mar 14. Eur J Vasc Endovasc Surg. 2015. PMID: 25784506
-
Surgical bypass vs endovascular treatment for patients with supra-aortic arterial occlusive disease due to Takayasu arteritis.J Vasc Surg. 2012 Mar;55(3):693-700. doi: 10.1016/j.jvs.2011.09.051. Epub 2011 Nov 25. J Vasc Surg. 2012. PMID: 22119246
-
Takayasu arteritis revisited: current diagnosis and treatment.Int J Cardiol. 2013 Sep 20;168(1):3-10. doi: 10.1016/j.ijcard.2013.01.022. Epub 2013 Feb 13. Int J Cardiol. 2013. PMID: 23415176 Review.
Cited by
-
Renal artery involvement is associated with increased morbidity but not mortality in Takayasu arteritis: a matched cohort study of 215 patients.Clin Rheumatol. 2024 Jan;43(1):67-80. doi: 10.1007/s10067-023-06829-9. Epub 2023 Dec 5. Clin Rheumatol. 2024. PMID: 38051415
-
Management of the renovascular disease in children with Takayasu arteritis.Pediatr Nephrol. 2015 Aug;30(8):1213-6. doi: 10.1007/s00467-015-3093-7. Epub 2015 May 16. Pediatr Nephrol. 2015. PMID: 25975436
-
Ischemic stroke as the first clinical manifestation of an initially undiagnosed case of Takayasu arteritis in a young woman from Ethiopia: A case report.SAGE Open Med Case Rep. 2024 Apr 6;12:2050313X241241190. doi: 10.1177/2050313X241241190. eCollection 2024. SAGE Open Med Case Rep. 2024. PMID: 38585421 Free PMC article.
-
Complex aortic arch repair in a patient with Takayasu's disease presenting with acute aortic dissection type Stanford A and complete collateral perfusion of the brain.Interact Cardiovasc Thorac Surg. 2016 Mar;22(3):384-6. doi: 10.1093/icvts/ivv336. Epub 2015 Dec 4. Interact Cardiovasc Thorac Surg. 2016. PMID: 26637541 Free PMC article.
-
MR and CT angiography in the diagnosis of vasculitides.BJR Open. 2023 Sep 25;5(1):20220020. doi: 10.1259/bjro.20220020. eCollection 2023. BJR Open. 2023. PMID: 37953869 Free PMC article. Review.
References
-
- Hotchi M. Pathological studies on Takayasu arteritis. Heart and Vessels. 1992;7(7):11–17. - PubMed
-
- Numano F, Kobayashi Y. Takayasu arteritis—beyond pulselessness. Internal Medicine. 1999;38(3):226–232. - PubMed
-
- Mason JC. Takayasu arteritis-advances in diagnosis and management. Nature Reviews Rheumatology. 2010;6(7):406–415. - PubMed
-
- Moriwaki R, Noda M, Yajima M, Sharma BK, Numano F. Clinical manifestations of Takayasu arteritis in India and Japan—new classification of angiographic findings. Angiology. 1997;48(5):369–379. - PubMed
-
- Ishikawa K. Natural history and classification of occlusive thromboaortopathy (Takayasu’s disease) Circulation. 1978;57(1):27–35. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
