

IL-17A mediates early post-transplant lesions after heterotopic trachea allotransplantation in Mice
- PMID: 23936171
- PMCID: PMC3728020
- DOI: 10.1371/journal.pone.0070236
IL-17A mediates early post-transplant lesions after heterotopic trachea allotransplantation in Mice
Abstract
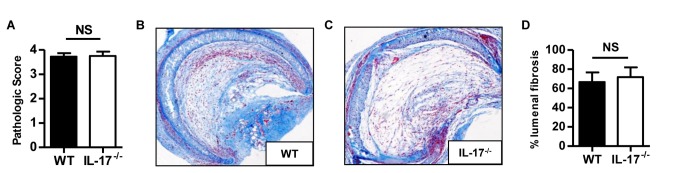
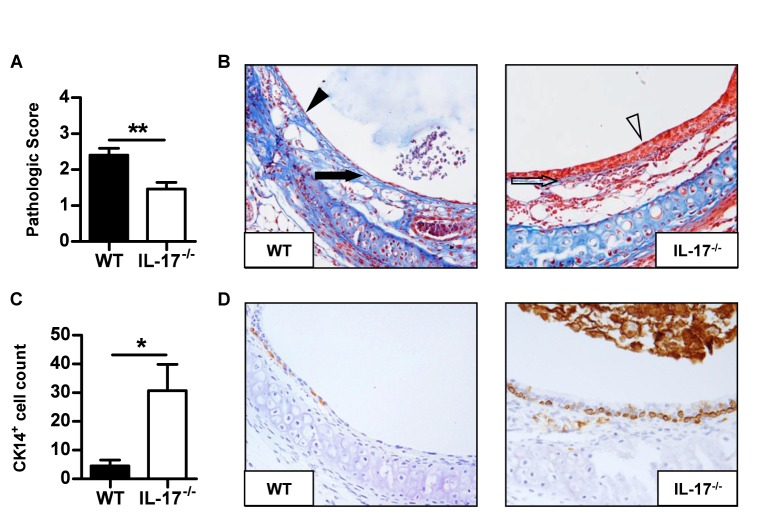
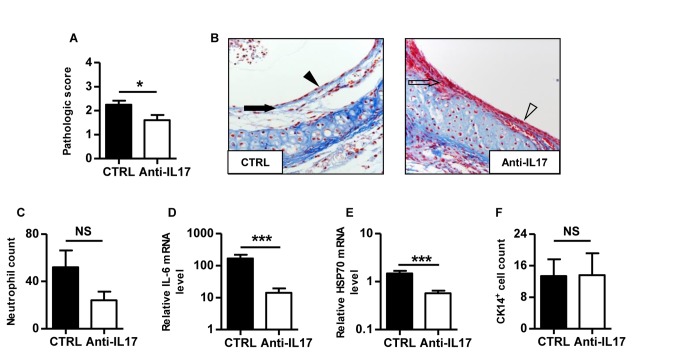
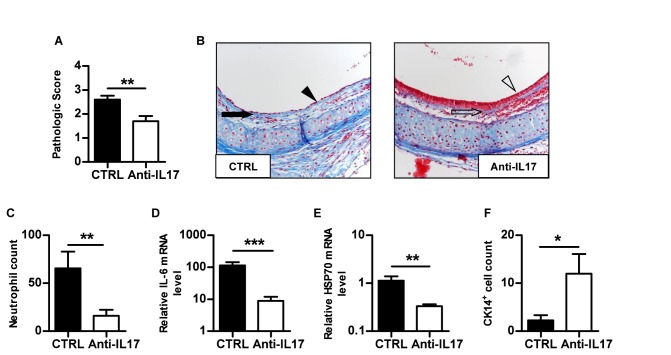
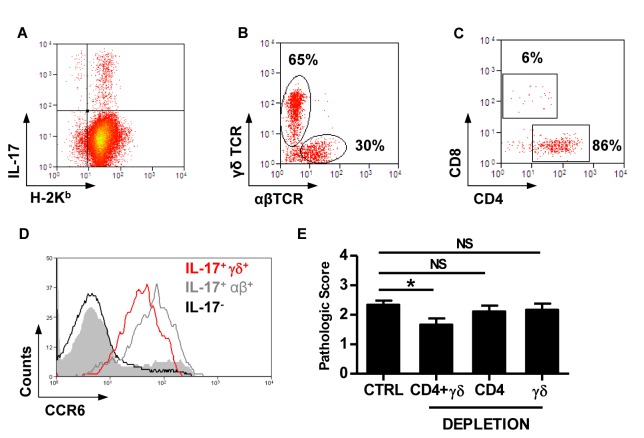
Primary graft dysfunction (PGD) and bronchiolitis obliterans (BO) are the leading causes of morbidity and mortality after lung transplantation. Reports from clinical and rodent models suggest the implication of IL-17A in either PGD or BO. We took advantage of the heterotopic trachea transplantation model in mice to study the direct role of IL-17A in post-transplant airway lesions. Across full MHC barrier, early lesions were controlled in IL-17A(-/-) or anti-IL17 treated recipients. In contrast, IL-17A deficiency did not prevent subsequent obliterative airway disease (OAD). Interestingly, this early protection occurred also in syngeneic grafts and was accompanied by a decrease in cellular stress, as attested by lower HSP70 mRNA levels, suggesting the involvement of IL-17A in ischemia-reperfusion injury (IRI). Furthermore, persistence of multipotent CK14(+) epithelial stem cells underlined allograft protection afforded by IL-17A deficiency or neutralisation. Recipient-derived γδ(+) and CD4(+) T cells were the major source of IL-17A. However, lesions still occurred in the absence of each subset, suggesting a high redundancy between the innate and adaptive IL-17A producing cells. Notably, a double depletion significantly diminished lesions. In conclusion, this work implicated IL-17A as mediator of early post-transplant airway lesions and could be considered as a potential therapeutic target in clinical transplantation.
Conflict of interest statement
Figures
Similar articles
-
CD4 T Cells but Not Th17 Cells Are Required for Mouse Lung Transplant Obliterative Bronchiolitis.Am J Transplant. 2015 Jul;15(7):1793-1804. doi: 10.1111/ajt.13215. Epub 2015 Mar 13. Am J Transplant. 2015. PMID: 25773063 Free PMC article.
-
IL-17A Is Critical for CD8+ T Effector Response in Airway Epithelial Injury After Transplantation.Transplantation. 2018 Dec;102(12):e483-e493. doi: 10.1097/TP.0000000000002452. Transplantation. 2018. PMID: 30211827
-
Cyclosporine A drives a Th17- and Th2-mediated posttransplant obliterative airway disease.Am J Transplant. 2013 Mar;13(3):611-20. doi: 10.1111/ajt.12067. Epub 2013 Jan 17. Am J Transplant. 2013. PMID: 23331973
-
The role of recipient derived interleukin-17A in a murine orthotopic lung transplant model of restrictive chronic lung allograft dysfunction.Transpl Immunol. 2016 Nov;39:10-17. doi: 10.1016/j.trim.2016.10.001. Epub 2016 Oct 11. Transpl Immunol. 2016. PMID: 27737799
-
Molecular mechanisms of chronic rejection following transplantation.Immunol Res. 2005;32(1-3):179-85. doi: 10.1385/IR:32:1-3:179. Immunol Res. 2005. PMID: 16106068 Review.
Cited by
-
IL-17A Contributes to Lung Fibrosis in a Model of Chronic Pulmonary Graft-versus-host Disease.Transplantation. 2019 Nov;103(11):2264-2274. doi: 10.1097/TP.0000000000002837. Transplantation. 2019. PMID: 31658231 Free PMC article.
-
Specific Donor HLA-DR Types Correlate With Altered Susceptibility to Development of Chronic Lung Allograft Dysfunction.Transplantation. 2018 Jul;102(7):1132-1138. doi: 10.1097/TP.0000000000002107. Transplantation. 2018. PMID: 29360666 Free PMC article.
-
CD4 T Cells but Not Th17 Cells Are Required for Mouse Lung Transplant Obliterative Bronchiolitis.Am J Transplant. 2015 Jul;15(7):1793-1804. doi: 10.1111/ajt.13215. Epub 2015 Mar 13. Am J Transplant. 2015. PMID: 25773063 Free PMC article.
-
SOCS3 overexpression in T cells ameliorates chronic airway obstruction in a murine heterotopic tracheal transplantation model.Surg Today. 2019 May;49(5):443-450. doi: 10.1007/s00595-018-1753-5. Epub 2019 Jan 7. Surg Today. 2019. PMID: 30617600
-
IL-17A neutralization fails to attenuate airway remodeling and potentiates a proinflammatory lung microenvironment in diacetyl-exposed rats.Am J Physiol Lung Cell Mol Physiol. 2023 Oct 1;325(4):L434-L446. doi: 10.1152/ajplung.00082.2023. Epub 2023 Aug 29. Am J Physiol Lung Cell Mol Physiol. 2023. PMID: 37642674 Free PMC article.
References
-
- Lodhi SA, Lamb KE, Meier-Kriesche HU (2011) Solid organ allograft survival improvement in the United States: the long-term does not mirror the dramatic short-term success. Am J Transplant 11: 1226-1235. doi:10.1111/j.1600-6143.2011.03539.x. PubMed: 21564524. - DOI - PubMed
-
- Lee JC, Christie JD (2009) Primary graft dysfunction. Proc Am Thorac Soc 6: 39-46. doi:10.1513/pats.200808-082GO. PubMed: 19131529. - DOI - PubMed
-
- Christie JD, Bellamy S, Ware LB, Lederer D, Hadjiliadis D et al. (2010) Construct validity of the definition of primary graft dysfunction after lung transplantation. J Heart Lung Transplant 29: 1231-1239. doi:10.1016/j.healun.2010.05.013. PubMed: 20655249. - DOI - PMC - PubMed
-
- Christie JD, Edwards LB, Kucheryavaya AY, Aurora P, Dobbels F et al. (2010) The Registry of the International Society for Heart and Lung Transplantation: twenty-seventh official adult lung and heart-lung transplant report--2010. J Heart Lung Transplant 29: 1104-1118. doi:10.1016/j.healun.2010.08.004. PubMed: 20870165. - DOI - PubMed
-
- Daud SA, Yusen RD, Meyers BF, Chakinala MM, Walter MJ et al. (2007) Impact of immediate primary lung allograft dysfunction on bronchiolitis obliterans syndrome. Am J Respir Crit Care Med 175: 507-513. doi:10.1164/rccm.200608-1079OC. PubMed: 17158279. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
