

Bioenergetics of the calf muscle in Friedreich ataxia patients measured by 31P-MRS before and after treatment with recombinant human erythropoietin
- PMID: 23922695
- PMCID: PMC3726701
- DOI: 10.1371/journal.pone.0069229
Bioenergetics of the calf muscle in Friedreich ataxia patients measured by 31P-MRS before and after treatment with recombinant human erythropoietin
Abstract
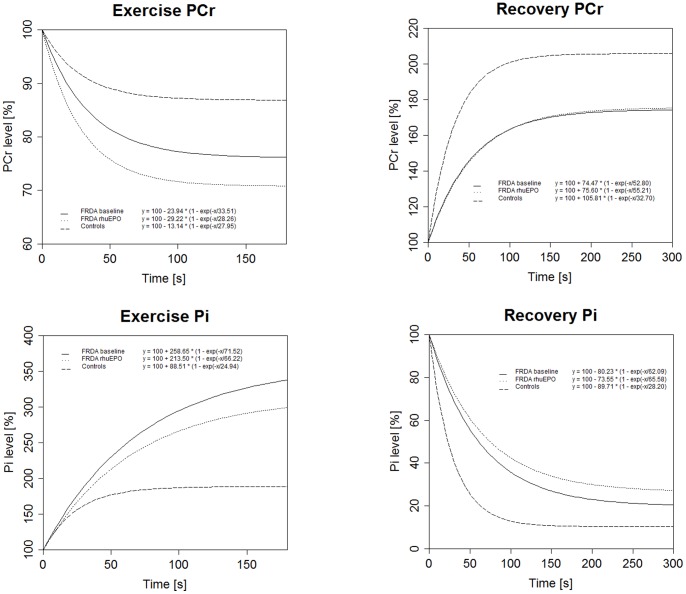
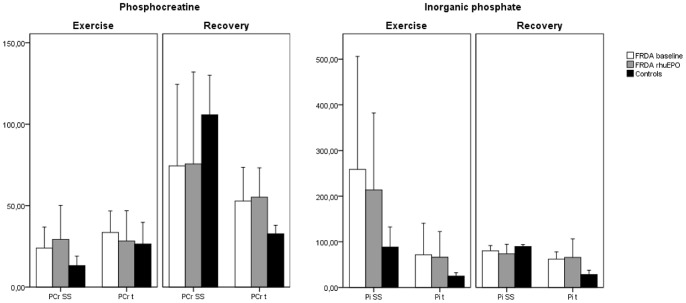
Friedreich ataxia (FRDA) is caused by a GAA repeat expansion in the FXN gene leading to reduced expression of the mitochondrial protein frataxin. Recombinant human erythropoietin (rhuEPO) is suggested to increase frataxin levels, alter mitochondrial function and improve clinical scores in FRDA patients. Aim of the present pilot study was to investigate mitochondrial metabolism of skeletal muscle tissue in FRDA patients and examine effects of rhuEPO administration by phosphorus 31 magnetic resonance spectroscopy (31P MRS). Seven genetically confirmed FRDA patients underwent 31P MRS of the calf muscles using a rest-exercise-recovery protocol before and after receiving 3000 IU of rhuEPO for eight weeks. FRDA patients showed more rapid phosphocreatine (PCr) depletion and increased accumulation of inorganic phosphate (Pi) during incremental exercise as compared to controls. After maximal exhaustive exercise prolonged regeneration of PCR and slowed decline in Pi can be seen in FRDA. PCr regeneration as hallmark of mitochondrial ATP production revealed correlation to activity of complex II/III of the respiratory chain and to demographic values. PCr and Pi kinetics were not influenced by rhuEPO administration. Our results confirm mitochondrial dysfunction and exercise intolerance due to impaired oxidative phosphorylation in skeletal muscle tissue of FRDA patients. MRS did not show improved mitochondrial bioenergetics after eight weeks of rhuEPO exposition in skeletal muscle tissue of FRDA patients.
Trial registration: EU Clinical Trials Register2008-000040-13.
Conflict of interest statement
Figures

Similar articles
-
Skeletal muscle involvement in friedreich ataxia and potential effects of recombinant human erythropoietin administration on muscle regeneration and neovascularization.J Neuropathol Exp Neurol. 2012 Aug;71(8):708-15. doi: 10.1097/NEN.0b013e31825fed76. J Neuropathol Exp Neurol. 2012. PMID: 22805773
-
Cellular bioenergetics after erythropoietin therapy in chronic renal failure.J Clin Invest. 1996 May 1;97(9):2101-10. doi: 10.1172/JCI118647. J Clin Invest. 1996. PMID: 8621800 Free PMC article.
-
Effects of erythropoietin on frataxin levels and mitochondrial function in Friedreich ataxia--a dose-response trial.Cerebellum. 2011 Dec;10(4):763-9. doi: 10.1007/s12311-011-0287-9. Cerebellum. 2011. PMID: 21597884 Clinical Trial.
-
Erythropoietin in Friedreich ataxia.J Neurochem. 2013 Aug;126 Suppl 1:80-7. doi: 10.1111/jnc.12301. J Neurochem. 2013. PMID: 23859343 Review.
-
Absolute quantification of phosphorus metabolite concentrations in human muscle in vivo by 31P MRS: a quantitative review.NMR Biomed. 2007 Oct;20(6):555-65. doi: 10.1002/nbm.1192. NMR Biomed. 2007. PMID: 17628042 Review.
Cited by
-
Skeletal muscle transcriptomics dissects the pathogenesis of Friedreich's ataxia.Hum Mol Genet. 2023 Jun 19;32(13):2241-2250. doi: 10.1093/hmg/ddad051. Hum Mol Genet. 2023. PMID: 37027192 Free PMC article.
-
Mitochondrial function is impaired in the skeletal muscle of pre-frail elderly.Sci Rep. 2018 Jun 4;8(1):8548. doi: 10.1038/s41598-018-26944-x. Sci Rep. 2018. PMID: 29867098 Free PMC article. Clinical Trial.
-
Impact of Drosophila Models in the Study and Treatment of Friedreich's Ataxia.Int J Mol Sci. 2018 Jul 7;19(7):1989. doi: 10.3390/ijms19071989. Int J Mol Sci. 2018. PMID: 29986523 Free PMC article. Review.
-
Therapeutic Biomarkers in Friedreich's Ataxia: a Systematic Review and Meta-analysis.Cerebellum. 2024 Jun;23(3):1184-1203. doi: 10.1007/s12311-023-01621-6. Epub 2023 Oct 27. Cerebellum. 2024. PMID: 37889470 Free PMC article.
-
Erythropoietin and Friedreich Ataxia: Time for a Reappraisal?Front Neurosci. 2019 Apr 24;13:386. doi: 10.3389/fnins.2019.00386. eCollection 2019. Front Neurosci. 2019. PMID: 31105516 Free PMC article. Review.
References
-
- Harding AE (1981) Friedreich's ataxia: a clinical and genetic study of 90 families with an analysis of early diagnostic criteria and intrafamilial clustering of clinical features. Brain 104: 589–620. - PubMed
-
- Beauchamp M, Labelle H, Duhaime M, Joncas J (1995) Natural history of muscle weakness in Friedreich's Ataxia and its relation to loss of ambulation. Clin Orthop Relat Res: 270–275. - PubMed
-
- Sival DA, Pouwels ME, Van Brederode A, Maurits NM, Verschuuren-Bemelmans CC, et al. (2011) In children with Friedreich ataxia, muscle and ataxia parameters are associated. Dev Med Child Neurol 53: 529–534. - PubMed
-
- Campuzano V, Montermini L, Molto MD, Pianese L, Cossee M, et al. (1996) Friedreich's ataxia: autosomal recessive disease caused by an intronic GAA triplet repeat expansion. Science 271: 1423–1427. - PubMed
-
- Pandolfo M, Pastore A (2009) The pathogenesis of Friedreich ataxia and the structure and function of frataxin. J Neurol 256 Suppl 19–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
