

Combination interventions to prevent HCV transmission among people who inject drugs: modeling the impact of antiviral treatment, needle and syringe programs, and opiate substitution therapy
- PMID: 23884064
- PMCID: PMC3722076
- DOI: 10.1093/cid/cit296
Combination interventions to prevent HCV transmission among people who inject drugs: modeling the impact of antiviral treatment, needle and syringe programs, and opiate substitution therapy
Erratum in
- Clin Infect Dis. 2014 Apr;58(8):1203
Abstract
Background: Interventions such as opiate substitution therapy (OST) and high-coverage needle and syringe programs (HCNSP) cannot substantially reduce hepatitis C virus (HCV) prevalence among people who inject drugs (PWID). HCV antiviral treatment may prevent onward transmission. We project the impact of combining OST, HCNSP, and antiviral treatment on HCV prevalence/incidence among PWID.
Methods: An HCV transmission model among PWID was used to project the combinations of OST, HCNSP, and antiviral treatment required to achieve different prevalence and incidence reductions within 10 years for 3 chronic prevalence scenarios and the impact of HCV treatment if only delivered through OST programs. Multivariate and univariate sensitivity analyses were performed.
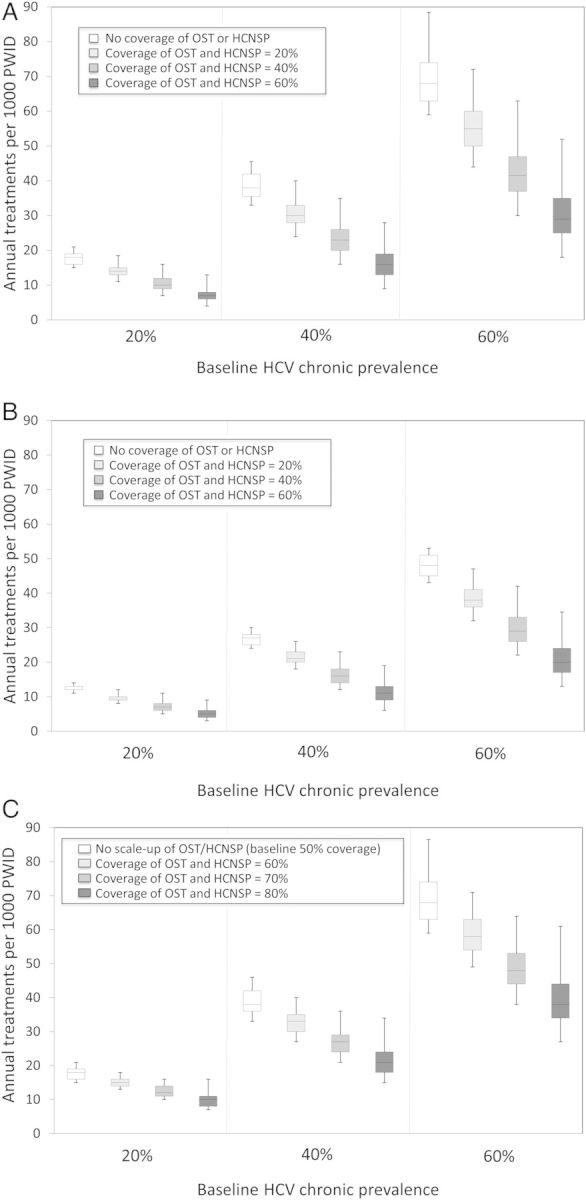
Results: Large reductions (>45%) in HCV chronic prevalence over 10 years require HCV antiviral treatment. Scaling up OST and HCNSP substantially reduces the treatment rate required to achieve specific HCV prevalence reductions. If OST and HCNSP coverage were increased to 40% each (no coverage at baseline), then annually treating 10, 23, or 42 per 1000 PWID over 10 years would halve prevalence for 20%, 40%, or 60% baseline chronic HCV prevalences, respectively. Approximately 30% fewer treatments are necessary with new direct-acting antivirals. If coverage of OST and HCNSP is 50% at baseline, similar prevalence reductions require higher treatment rates for the same OST and HCNSP coverage.
Conclusions: Combining antiviral treatment with OST with HCNSP is critical for achieving substantial reductions (>50%) in HCV chronic prevalence over 10 years. Empirical studies are required on how best to scale up antiviral treatment and combine treatment with other interventions.
Figures


Similar articles
-
Model projections on the impact of HCV treatment in the prevention of HCV transmission among people who inject drugs in Europe.J Hepatol. 2018 Mar;68(3):402-411. doi: 10.1016/j.jhep.2017.10.010. Epub 2018 Jan 8. J Hepatol. 2018. PMID: 29080808 Free PMC article.
-
Impact of current and scaled-up levels of hepatitis C prevention and treatment interventions for people who inject drugs in three UK settings-what is required to achieve the WHO's HCV elimination targets?Addiction. 2018 May 17;113(9):1727-38. doi: 10.1111/add.14217. Online ahead of print. Addiction. 2018. PMID: 29774607 Free PMC article.
-
Modelling the impact of a national scale-up of interventions on hepatitis C virus transmission among people who inject drugs in Scotland.Addiction. 2018 Nov;113(11):2118-2131. doi: 10.1111/add.14267. Epub 2018 Jul 10. Addiction. 2018. PMID: 29781207 Free PMC article.
-
Needle syringe programmes and opioid substitution therapy for preventing hepatitis C transmission in people who inject drugs.Cochrane Database Syst Rev. 2017 Sep 18;9(9):CD012021. doi: 10.1002/14651858.CD012021.pub2. Cochrane Database Syst Rev. 2017. PMID: 28922449 Free PMC article. Review.
-
Global, regional, and country-level coverage of interventions to prevent and manage HIV and hepatitis C among people who inject drugs: a systematic review.Lancet Glob Health. 2017 Dec;5(12):e1208-e1220. doi: 10.1016/S2214-109X(17)30373-X. Epub 2017 Oct 23. Lancet Glob Health. 2017. PMID: 29074410 Free PMC article. Review.
Cited by
-
A public health approach to hepatitis C control in low- and middle-income countries.PLoS Med. 2015 Mar 10;12(3):e1001795. doi: 10.1371/journal.pmed.1001795. eCollection 2015 Mar. PLoS Med. 2015. PMID: 25757228 Free PMC article.
-
The hepatitis C virus epidemics in key populations (including people who inject drugs, prisoners and MSM): the use of direct-acting antivirals as treatment for prevention.Curr Opin HIV AIDS. 2015 Sep;10(5):374-80. doi: 10.1097/COH.0000000000000179. Curr Opin HIV AIDS. 2015. PMID: 26248124 Free PMC article. Review.
-
Missed opportunities for prevention and treatment of hepatitis C among persons with HIV/HCV coinfection.AIDS Care. 2020 Jul;32(7):921-929. doi: 10.1080/09540121.2019.1668533. Epub 2019 Sep 23. AIDS Care. 2020. PMID: 31547683 Free PMC article.
-
The Decade-Long Chinese Methadone Maintenance Therapy Yields Large Population and Economic Benefits for Drug Users in Reducing Harm, HIV and HCV Disease Burden.Front Public Health. 2019 Nov 12;7:327. doi: 10.3389/fpubh.2019.00327. eCollection 2019. Front Public Health. 2019. PMID: 31781529 Free PMC article.
-
Hepatitis C Within a Single Health System: Progression Along the Cascade to Cure Is Higher for Those With Substance Misuse When Linked to a Clinic With Embedded Support Services.Open Forum Infect Dis. 2018 Sep 20;5(9):ofy202. doi: 10.1093/ofid/ofy202. eCollection 2018 Sep. Open Forum Infect Dis. 2018. PMID: 30255113 Free PMC article.
References
-
- Shepard CW, Finelli L, Alter MJ. Global epidemiology of hepatitis C virus infection. Lancet Infec Dis. 2005;5:558–67. - PubMed
-
- De Angelis D, et al. An evidence synthesis approach to estimating hepatitis C prevalence in England and Wales. Stat Methods Med Res. 2009;18:361–79. - PubMed
-
- Turner K, et al. The impact of needle and syringe provision and opiate substitution therapy on the incidence of hepatitis C virus in injecting drug users: pooling of UK evidence. Addiction. 2011;106:1978–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
