

Intestinal permeability defects: is it time to treat?
- PMID: 23851019
- PMCID: PMC3758766
- DOI: 10.1016/j.cgh.2013.07.001
Intestinal permeability defects: is it time to treat?
Abstract
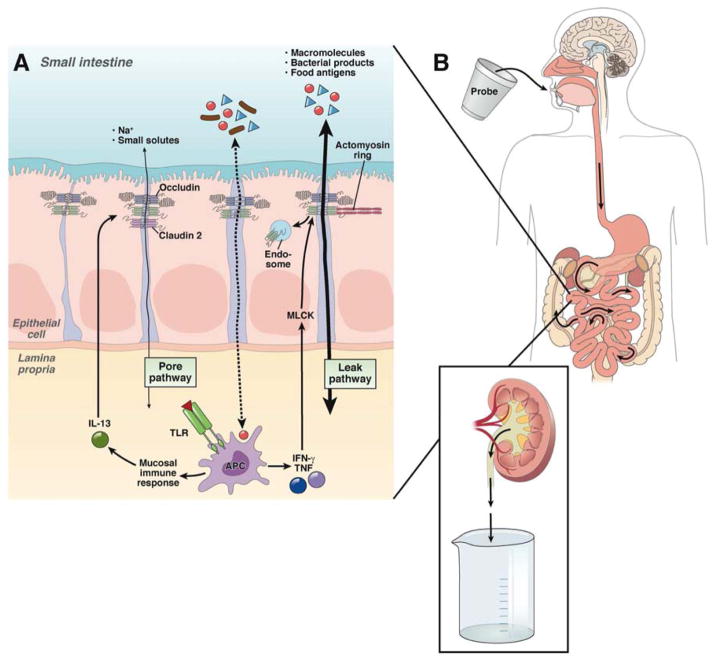
An essential role of the intestinal epithelium is to separate luminal contents from the interstitium, a function primarily determined by the integrity of the epithelium and the tight junction that seals the paracellular space. Intestinal tight junctions are selectively permeable, and intestinal permeability can be increased physiologically in response to luminal nutrients or pathologically by mucosal immune cells and cytokines, the enteric nervous system, and pathogens. Compromised intestinal barrier function is associated with an array of clinical conditions, both intestinal and systemic. Although most available data are correlative, some studies support a model where cycles of increased intestinal permeability, intestinal immune activation, and subsequent immune-mediated barrier loss contribute to disease progression. This model is applicable to intestinal and systemic diseases. However, it has not been proven, and both mechanistic and therapeutic studies are ongoing. Nevertheless, the correlation between increased intestinal permeability and disease has caught the attention of the public, leading to a rise in popularity of the diagnosis of "leaky gut syndrome," which encompasses a range of systemic disorders. Proponents claim that barrier restoration will cure underlying disease, but this has not been demonstrated in clinical trials. Moreover, human and mouse studies show that intestinal barrier loss alone is insufficient to initiate disease. It is therefore uncertain whether increased permeability in these patients is a cause or effect of the underlying disorder. Although drug targets that may mediate barrier restoration have been proposed, none have been proven effective. As such, current treatments for barrier dysfunction should target the underlying disease.
Keywords: CA-MLCK; CD; Claudin; Crohn’s disease; GVHD; Graft vs Host Disease; IBD; IBS; IL; Inflammatory Bowel Disease; Irritable Bowel Syndrome; Leaky Gut Syndrome; MLCK; Myosin Light Chain Kinase; TNF; Tight Junction; constitutively active–myosin light chain kinase; graft-versus-host disease; inflammatory bowel disease; interleukin; irritable bowel syndrome; myosin light chain kinase; tumor necrosis factor.
Copyright © 2013 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Myosin light chain kinase regulates intestinal permeability of mucosal homeostasis in Crohn's disease.Expert Rev Clin Immunol. 2020 Dec;16(12):1127-1141. doi: 10.1080/1744666X.2021.1850269. Epub 2020 Dec 29. Expert Rev Clin Immunol. 2020. PMID: 33183108 Review.
-
Epithelial myosin light chain kinase activation induces mucosal interleukin-13 expression to alter tight junction ion selectivity.J Biol Chem. 2010 Apr 16;285(16):12037-46. doi: 10.1074/jbc.M109.064808. Epub 2010 Feb 22. J Biol Chem. 2010. PMID: 20177070 Free PMC article.
-
Interleukin-18 facilitates neutrophil transmigration via myosin light chain kinase-dependent disruption of occludin, without altering epithelial permeability.Am J Physiol Gastrointest Liver Physiol. 2012 Feb 1;302(3):G343-51. doi: 10.1152/ajpgi.00202.2011. Epub 2011 Dec 1. Am J Physiol Gastrointest Liver Physiol. 2012. PMID: 22135309
-
Myosin light chain kinase mediates intestinal barrier dysfunction via occludin endocytosis during anoxia/reoxygenation injury.Am J Physiol Cell Physiol. 2016 Dec 1;311(6):C996-C1004. doi: 10.1152/ajpcell.00113.2016. Epub 2016 Oct 19. Am J Physiol Cell Physiol. 2016. PMID: 27760753
-
Abnormal Barrier Function in Gastrointestinal Disorders.Handb Exp Pharmacol. 2017;239:193-217. doi: 10.1007/164_2016_107. Handb Exp Pharmacol. 2017. PMID: 27995392 Review.
Cited by
-
A leaky human colon model reveals uncoupled apical/basal cytotoxicity in early Clostridioides difficile toxin exposure.Am J Physiol Gastrointest Liver Physiol. 2023 Apr 1;324(4):G262-G280. doi: 10.1152/ajpgi.00251.2022. Epub 2023 Feb 7. Am J Physiol Gastrointest Liver Physiol. 2023. PMID: 36749911 Free PMC article.
-
Intestinal Barrier Function and Immune Homeostasis Are Missing Links in Obesity and Type 2 Diabetes Development.Front Endocrinol (Lausanne). 2022 Jan 25;12:833544. doi: 10.3389/fendo.2021.833544. eCollection 2021. Front Endocrinol (Lausanne). 2022. PMID: 35145486 Free PMC article. Review.
-
Food as Treatment of Inflammatory Bowel Diseases.Infect Immun. 2022 May 19;90(5):e0058321. doi: 10.1128/iai.00583-21. Epub 2022 May 11. Infect Immun. 2022. PMID: 35323020 Free PMC article. Review.
-
QingBai decoction regulates intestinal permeability of dextran sulphate sodium-induced colitis through the modulation of notch and NF-κB signalling.Cell Prolif. 2019 Mar;52(2):e12547. doi: 10.1111/cpr.12547. Epub 2019 Jan 18. Cell Prolif. 2019. PMID: 30657238 Free PMC article.
-
Gastrointestinal microbiota alteration induced by Mucor circinelloides in a murine model.J Microbiol. 2019 Jun;57(6):509-520. doi: 10.1007/s12275-019-8682-x. Epub 2019 May 27. J Microbiol. 2019. PMID: 31012059 Free PMC article.
References
-
- Turner JR. Intestinal mucosal barrier function in health and disease. Nat Rev Immunol. 2009;9:799–809. - PubMed
-
- Van der Sluis M, De Koning BA, De Bruijn AC, et al. Muc2-deficient mice spontaneously develop colitis, indicating that MUC2 is critical for colonic protection. Gastroenterology. 2006;131:117–29. - PubMed
-
- Kottra G, Fromter E. Functional properties of the paracellular pathway in some leaky epithelia. J Exp Biol. 1983;106:217–29. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
