

Targeting the "Rising DAMP" during a Francisella tularensis Infection
- PMID: 23796927
- PMCID: PMC3754292
- DOI: 10.1128/AAC.01885-12
Targeting the "Rising DAMP" during a Francisella tularensis Infection
Abstract
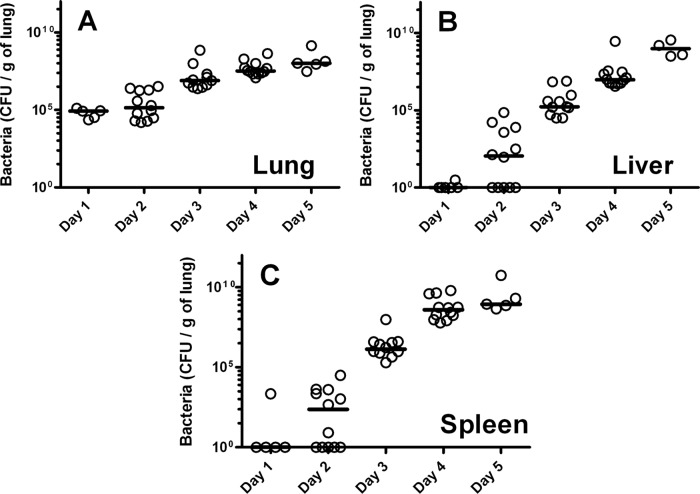
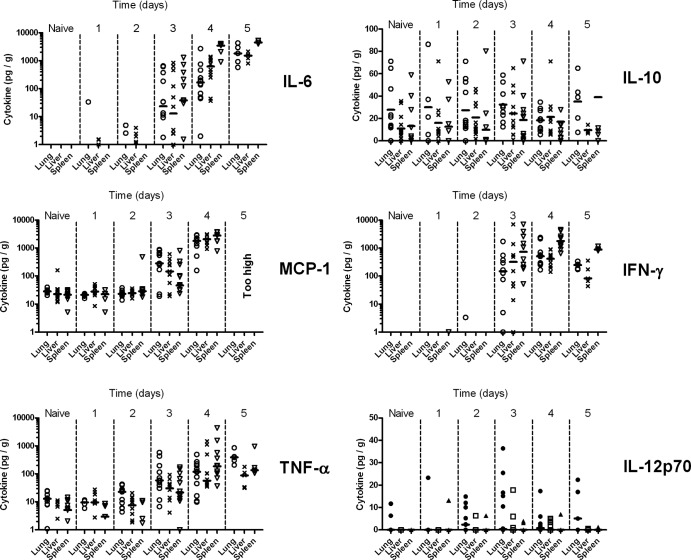
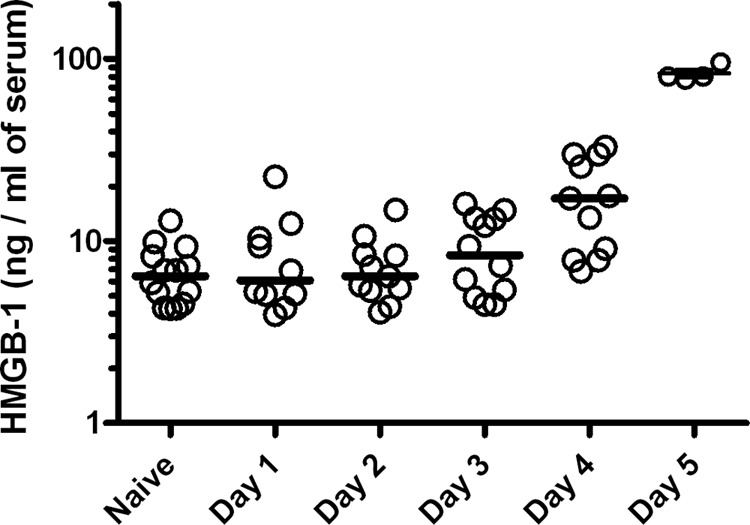
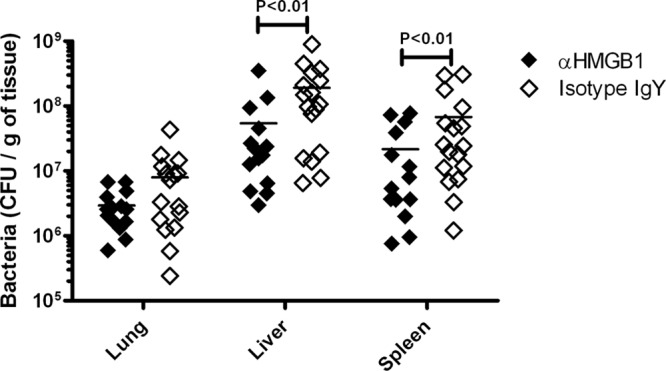
Antibiotic efficacy is greatly enhanced the earlier it is administered following infection with a bacterial pathogen. However, in a clinical setting antibiotic treatment usually commences following the onset of symptoms, which in some cases (e.g., biothreat agents) may be too late. In a BALB/c murine intranasal model of infection for Francisella tularensis SCHU S4 infection, we demonstrate during a time course experiment that proinflammatory cytokines and the damage-associated molecular pattern HMGB1 were not significantly elevated above naive levels in tissue or sera until 72 h postinfection. HMGB1 was identified as a potential therapeutic target that could extend the window of opportunity for the treatment of tularemia with antibiotics. Antibodies to HMGB1 were administered in conjunction with a delayed/suboptimal levofloxacin treatment of F. tularensis We found in the intranasal model of infection that treatment with anti-HMGB1 antibody, compared to an isotype IgY control antibody, conferred a significant survival benefit and decreased bacterial loads in the spleen and liver but not the lung (primary loci of infection) 4 days into infection. We also observed an increase in the production of gamma interferon in all tested organs. These data demonstrate that treatment with anti-HMGB1 antibody is beneficial in enhancing the effectiveness of current antibiotics in treating tularemia. Strategies of this type, involving antibiotics in combination with immunomodulatory drugs, are likely to be essential for the development of a postexposure therapeutic for intracellular pathogens.
Copyright © 2013, American Society for Microbiology. All Rights Reserved.
Figures
Similar articles
-
A Bioluminescent Francisella tularensis SCHU S4 Strain Enables Noninvasive Tracking of Bacterial Dissemination and the Evaluation of Antibiotics in an Inhalational Mouse Model of Tularemia.Antimicrob Agents Chemother. 2016 Nov 21;60(12):7206-7215. doi: 10.1128/AAC.01586-16. Print 2016 Dec. Antimicrob Agents Chemother. 2016. PMID: 27671061 Free PMC article.
-
Monophosphoryl Lipid A Enhances Efficacy of a Francisella tularensis LVS-Catanionic Nanoparticle Subunit Vaccine against F. tularensis Schu S4 Challenge by Augmenting both Humoral and Cellular Immunity.Clin Vaccine Immunol. 2017 Mar 6;24(3):e00574-16. doi: 10.1128/CVI.00574-16. Print 2017 Mar. Clin Vaccine Immunol. 2017. PMID: 28077440 Free PMC article.
-
Levofloxacin rescues mice from lethal intra-nasal infections with virulent Francisella tularensis and induces immunity and production of protective antibody.Vaccine. 2008 Dec 9;26(52):6874-82. doi: 10.1016/j.vaccine.2008.09.077. Epub 2008 Oct 16. Vaccine. 2008. PMID: 18930100 Free PMC article.
-
Characterization of Schu S4 aro mutants as live attenuated tularemia vaccine candidates.Virulence. 2020 Dec;11(1):283-294. doi: 10.1080/21505594.2020.1746557. Virulence. 2020. PMID: 32241221 Free PMC article.
-
Contributions of TolC Orthologs to Francisella tularensis Schu S4 Multidrug Resistance, Modulation of Host Cell Responses, and Virulence.Infect Immun. 2019 Mar 25;87(4):e00823-18. doi: 10.1128/IAI.00823-18. Print 2019 Apr. Infect Immun. 2019. PMID: 30670554 Free PMC article.
Cited by
-
A Bioluminescent Francisella tularensis SCHU S4 Strain Enables Noninvasive Tracking of Bacterial Dissemination and the Evaluation of Antibiotics in an Inhalational Mouse Model of Tularemia.Antimicrob Agents Chemother. 2016 Nov 21;60(12):7206-7215. doi: 10.1128/AAC.01586-16. Print 2016 Dec. Antimicrob Agents Chemother. 2016. PMID: 27671061 Free PMC article.
-
Stochastic dynamics of Francisella tularensis infection and replication.PLoS Comput Biol. 2020 Jun 1;16(6):e1007752. doi: 10.1371/journal.pcbi.1007752. eCollection 2020 Jun. PLoS Comput Biol. 2020. PMID: 32479491 Free PMC article.
-
Mitogen-activated protein kinases (MAPKs) are modulated during Francisella tularensis infection, but inhibition of extracellular-signal-regulated kinases (ERKs) is of limited therapeutic benefit.Eur J Clin Microbiol Infect Dis. 2016 Dec;35(12):2015-2024. doi: 10.1007/s10096-016-2754-1. Epub 2016 Oct 6. Eur J Clin Microbiol Infect Dis. 2016. PMID: 27714591 Free PMC article.
-
Border Patrol Gone Awry: Lung NKT Cell Activation by Francisella tularensis Exacerbates Tularemia-Like Disease.PLoS Pathog. 2015 Jun 11;11(6):e1004975. doi: 10.1371/journal.ppat.1004975. eCollection 2015 Jun. PLoS Pathog. 2015. PMID: 26068662 Free PMC article.
-
Modeling early events in Francisella tularensis pathogenesis.Front Cell Infect Microbiol. 2014 Dec 11;4:169. doi: 10.3389/fcimb.2014.00169. eCollection 2014. Front Cell Infect Microbiol. 2014. PMID: 25566509 Free PMC article.
References
-
- D'Elia R, Jenner DC, Laws TR, Stokes MGM, Jackson MC, Essex-Lopresti AE, Atkins HS. 2011. Inhibition of Francisella tularensis LVS infection of macrophages results in a reduced inflammatory response: evaluation of a therapeutic strategy for intracellular bacteria. FEMS Immunol. Med. Microbiol. 62:348–361 - PubMed
-
- Dennis DT, Inglesby TV, Henderson DA, Bartlett JG, Ascher MS, Eitzen E, Fine AD, Friedlander AM, Hauer J, Layton M, Lillibridge SR, Mcdade JE, Osterholm MT, O'Toole T, Parker G, Perl TM, Russell PK, Tonat K. 2001. Tularemia as a biological weapon—medical and public health management. JAMA 285:2763–2773 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
