

Androgen receptor functions in castration-resistant prostate cancer and mechanisms of resistance to new agents targeting the androgen axis
- PMID: 23752196
- PMCID: PMC4890635
- DOI: 10.1038/onc.2013.235
Androgen receptor functions in castration-resistant prostate cancer and mechanisms of resistance to new agents targeting the androgen axis
Abstract
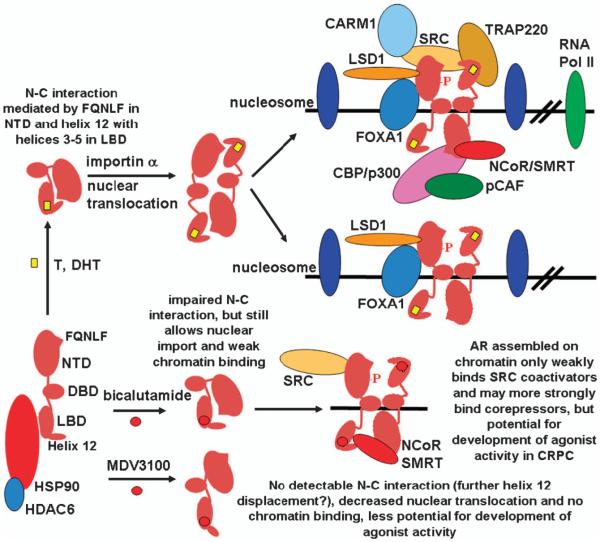
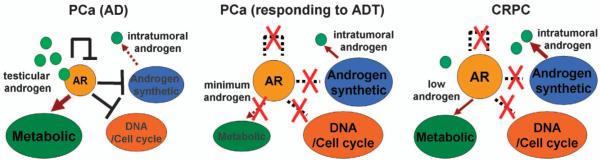
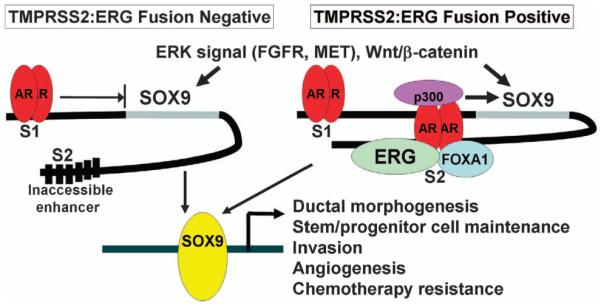
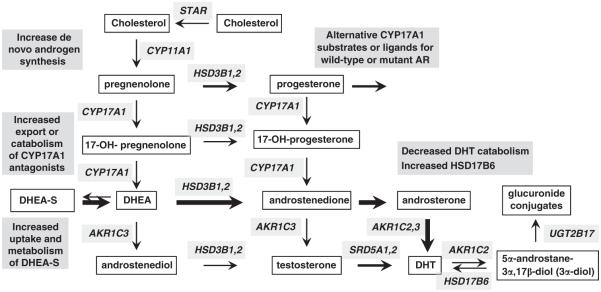
The metabolic functions of androgen receptor (AR) in normal prostate are circumvented in prostate cancer (PCa) to drive tumor growth, and the AR also can acquire new growth-promoting functions during PCa development and progression through genetic and epigenetic mechanisms. Androgen deprivation therapy (ADT, surgical or medical castration) is the standard treatment for metastatic PCa, but patients invariably relapse despite castrate androgen levels (castration-resistant PCa, CRPC). Early studies from many groups had shown that AR was highly expressed and transcriptionally active in CRPC, and indicated that steroids from the adrenal glands were contributing to this AR activity. More recent studies showed that CRPC cells had increased expression of enzymes mediating androgen synthesis from adrenal steroids, and could synthesize androgens de novo from cholesterol. Phase III clinical trials showing a survival advantage in CRPC for treatment with abiraterone (inhibitor of the enzyme CYP17A1 required for androgen synthesis that markedly reduces androgens and precursor steroids) and for enzalutamide (new AR antagonist) have now confirmed that AR activity driven by residual androgens makes a major contribution to CRPC, and led to the recent Food and Drug Administration approval of both agents. Unfortunately, patients treated with these agents for advanced CRPC generally relapse within a year and AR appears to be active in the relapsed tumors, but the molecular mechanisms mediating intrinsic or acquired resistance to these AR-targeted therapies remain to be defined. This review outlines AR functions that contribute to PCa development and progression, the roles of intratumoral androgen synthesis and AR structural alterations in driving AR activity in CRPC, mechanisms of action for abiraterone and enzalutamide, and possible mechanisms of resistance to these agents.
Figures
Similar articles
-
Abiraterone switches castration-resistant prostate cancer dependency from adrenal androgens towards androgen receptor variants and glucocorticoid receptor signalling.Prostate. 2022 Apr;82(5):505-516. doi: 10.1002/pros.24297. Epub 2022 Jan 17. Prostate. 2022. PMID: 35037287 Free PMC article.
-
A bypass mechanism of abiraterone-resistant prostate cancer: Accumulating CYP17A1 substrates activate androgen receptor signaling.Prostate. 2019 Jun;79(9):937-948. doi: 10.1002/pros.23799. Epub 2019 Apr 24. Prostate. 2019. PMID: 31017696 Free PMC article.
-
Androgen receptors in hormone-dependent and castration-resistant prostate cancer.Pharmacol Ther. 2013 Dec;140(3):223-38. doi: 10.1016/j.pharmthera.2013.07.003. Epub 2013 Jul 13. Pharmacol Ther. 2013. PMID: 23859952 Review.
-
Androgen receptor-dependent and -independent mechanisms driving prostate cancer progression: Opportunities for therapeutic targeting from multiple angles.Oncotarget. 2017 Jan 10;8(2):3724-3745. doi: 10.18632/oncotarget.12554. Oncotarget. 2017. PMID: 27741508 Free PMC article. Review.
-
A novel nonsense mutation in androgen receptor confers resistance to CYP17 inhibitor treatment in prostate cancer.Oncotarget. 2017 Jan 24;8(4):6796-6808. doi: 10.18632/oncotarget.14296. Oncotarget. 2017. PMID: 28036278 Free PMC article.
Cited by
-
Identification of long non-coding RNAs in advanced prostate cancer associated with androgen receptor splicing factors.Commun Biol. 2020 Jul 23;3(1):393. doi: 10.1038/s42003-020-01120-y. Commun Biol. 2020. PMID: 32704143 Free PMC article.
-
Early upregulation of AR and steroidogenesis enzyme expression after 3 months of androgen-deprivation therapy.BMC Urol. 2020 Jun 19;20(1):71. doi: 10.1186/s12894-020-00627-0. BMC Urol. 2020. PMID: 32560654 Free PMC article.
-
Increased AR expression in castration-resistant prostate cancer rapidly induces AR signaling reprogramming with the collaboration of EZH2.Front Oncol. 2022 Nov 3;12:1021845. doi: 10.3389/fonc.2022.1021845. eCollection 2022. Front Oncol. 2022. PMID: 36408179 Free PMC article.
-
Activation of GPR56, a novel adhesion GPCR, is necessary for nuclear androgen receptor signaling in prostate cells.PLoS One. 2020 Sep 3;15(9):e0226056. doi: 10.1371/journal.pone.0226056. eCollection 2020. PLoS One. 2020. PMID: 32881870 Free PMC article.
-
Lysine methyltransferase SMYD2 enhances androgen receptor signaling to modulate CRPC cell resistance to enzalutamide.Oncogene. 2024 Mar;43(10):744-757. doi: 10.1038/s41388-024-02945-1. Epub 2024 Jan 19. Oncogene. 2024. PMID: 38243079
References
-
- Mahoney EM, Harrison JH. Bilateral adrenalectomy for palliative treatment of prostatic cancer. J Urol. 1972;108:936–938. - PubMed
-
- Small EJ, Halabi S, Dawson NA, Stadler WM, Rini BI, Picus J, et al. Antiandrogen withdrawal alone or in combination with ketoconazole in androgen-independent prostate cancer patients: a phase III trial (CALGB 9583) J Clin Oncol. 2004;22:1025–1033. - PubMed
-
- Yap TA, Carden CP, Attard G, de Bono JS. Targeting CYP17: established and novel approaches in prostate cancer. Curr Opin Pharmacol. 2008;8:449–457. - PubMed
-
- Eisenberger MA, Blumenstein BA, Crawford ED, Miller G, McLeod DG, Loehrer PJ, et al. Bilateral orchiectomy with or without flutamide for metastatic prostate cancer. N Engl J Med. 1998;339:1036–1042. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
