

High myeloperoxidase positive cell infiltration in colorectal cancer is an independent favorable prognostic factor
- PMID: 23734221
- PMCID: PMC3667167
- DOI: 10.1371/journal.pone.0064814
High myeloperoxidase positive cell infiltration in colorectal cancer is an independent favorable prognostic factor
Abstract
Background: Colorectal cancer (CRC) infiltration by adaptive immune system cells correlates with favorable prognosis. The role of the innate immune system is still debated. Here we addressed the prognostic impact of CRC infiltration by neutrophil granulocytes (NG).
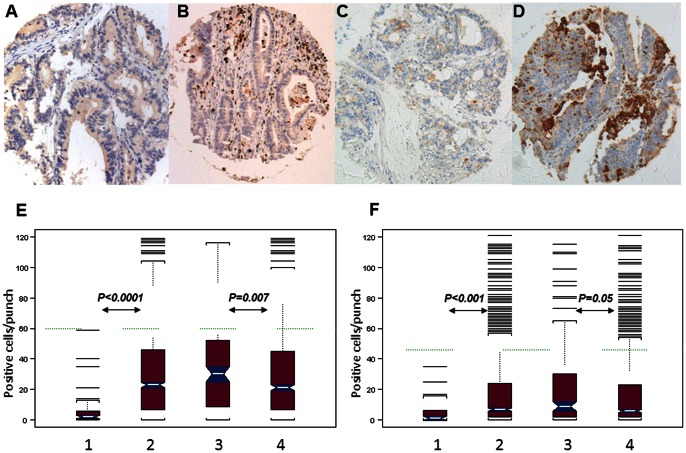
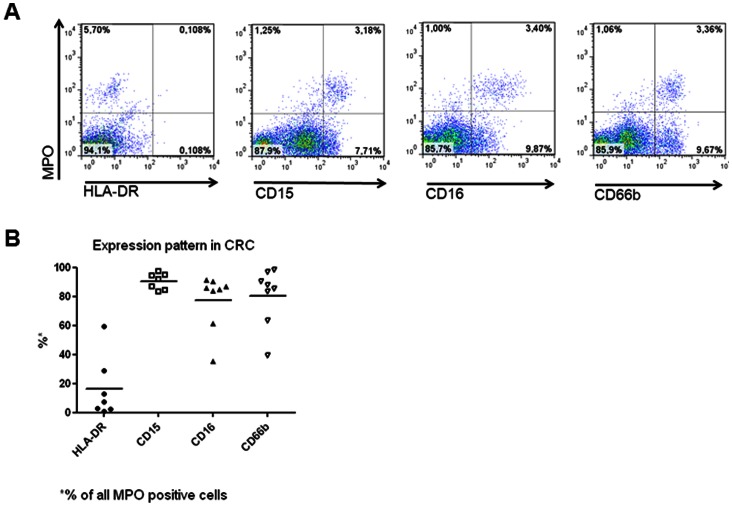
Methods: A TMA including healthy mucosa and clinically annotated CRC specimens (n = 1491) was stained with MPO and CD15 specific antibodies. MPO+ and CD15+ positive immune cells were counted by three independent observers. Phenotypic profiles of CRC infiltrating MPO+ and CD15+ cells were validated by flow cytometry on cell suspensions derived from enzymatically digested surgical specimens. Survival analysis was performed by splitting randomized data in training and validation subsets.
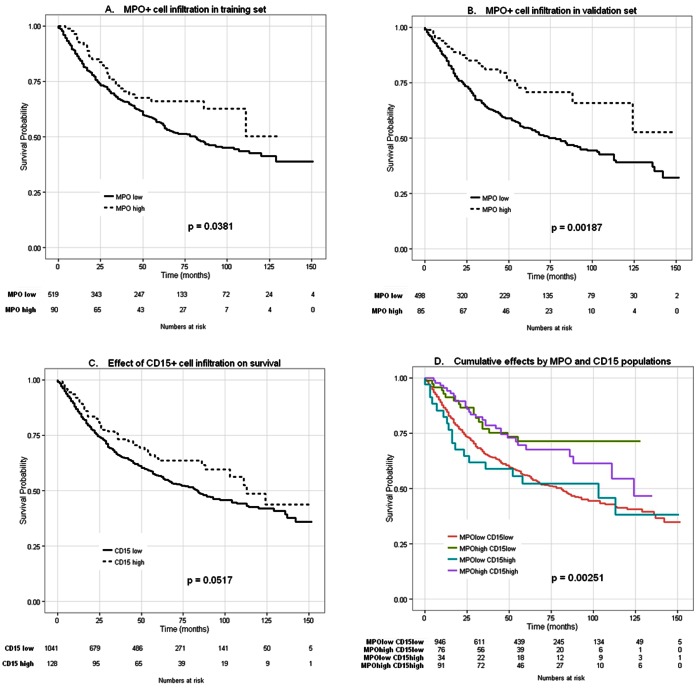
Results: MPO+ and CD15+ cell infiltration were significantly correlated (p<0.0001; r = 0.76). However, only high density of MPO+ cell infiltration was associated with significantly improved survival in training (P = 0.038) and validation (P = 0.002) sets. In multivariate analysis including T and N stage, vascular invasion, tumor border configuration and microsatellite instability status, MPO+ cell infiltration proved an independent prognostic marker overall (P = 0.004; HR = 0.65; CI:±0.15) and in both training (P = 0.048) and validation (P = 0.036) sets. Flow-cytometry analysis of CRC cell suspensions derived from clinical specimens showed that while MPO+ cells were largely CD15+/CD66b+, sizeable percentages of CD15+ and CD66b+ cells were MPO-.
Conclusions: High density MPO+ cell infiltration is a novel independent favorable prognostic factor in CRC.
Conflict of interest statement
Figures
Similar articles
-
The Interplay Between Neutrophils and CD8+ T Cells Improves Survival in Human Colorectal Cancer.Clin Cancer Res. 2017 Jul 15;23(14):3847-3858. doi: 10.1158/1078-0432.CCR-16-2047. Epub 2017 Jan 20. Clin Cancer Res. 2017. PMID: 28108544
-
Neutrophil infiltration is a favorable prognostic factor in early stages of colon cancer.Hum Pathol. 2017 Oct;68:193-202. doi: 10.1016/j.humpath.2017.08.028. Epub 2017 Sep 4. Hum Pathol. 2017. PMID: 28882699
-
Increased intratumoral neutrophil in colorectal carcinomas correlates closely with malignant phenotype and predicts patients' adverse prognosis.PLoS One. 2012;7(1):e30806. doi: 10.1371/journal.pone.0030806. Epub 2012 Jan 25. PLoS One. 2012. PMID: 22295111 Free PMC article.
-
Tumor-associated neutrophils as a new prognostic factor in cancer: a systematic review and meta-analysis.PLoS One. 2014 Jun 6;9(6):e98259. doi: 10.1371/journal.pone.0098259. eCollection 2014. PLoS One. 2014. PMID: 24906014 Free PMC article. Review.
-
Immune cells: plastic players along colorectal cancer progression.J Cell Mol Med. 2013 Sep;17(9):1088-95. doi: 10.1111/jcmm.12117. J Cell Mol Med. 2013. PMID: 24151976 Free PMC article. Review.
Cited by
-
Improving anticancer effect of aPD-L1 through lowering neutrophil infiltration by PLAG in tumor implanted with MB49 mouse urothelial carcinoma.BMC Cancer. 2022 Jul 4;22(1):727. doi: 10.1186/s12885-022-09815-7. BMC Cancer. 2022. PMID: 35787261 Free PMC article.
-
Tumor-derived granzyme B-expressing neutrophils acquire antitumor potential after lipid A treatment.Oncotarget. 2018 Jun 19;9(47):28364-28378. doi: 10.18632/oncotarget.25342. eCollection 2018 Jun 19. Oncotarget. 2018. PMID: 29983866 Free PMC article.
-
Role of KIR and CD16A genotypes in colorectal carcinoma genetic risk and clinical stage.J Transl Med. 2016 Aug 12;14(1):239. doi: 10.1186/s12967-016-1001-y. J Transl Med. 2016. PMID: 27519478 Free PMC article.
-
The Generation and Identity of Human Myeloid-Derived Suppressor Cells.Front Oncol. 2020 Feb 7;10:109. doi: 10.3389/fonc.2020.00109. eCollection 2020. Front Oncol. 2020. PMID: 32117758 Free PMC article. Review.
-
Prognostic Value of the Expression of DNA Repair-Related Biomarkers Mediated by Alcohol in Gastric Cancer Patients.Am J Pathol. 2018 Feb;188(2):367-377. doi: 10.1016/j.ajpath.2017.10.010. Epub 2018 Jan 10. Am J Pathol. 2018. PMID: 29331492 Free PMC article.
References
-
- Wood LD, Parsons DW, Jones S, Lin J, Sjoblom T, et al. (2007) The genomic landscapes of human breast and colorectal cancers. Science 318: 1108–1113. - PubMed
-
- Hanahan D, Weinberg RA (2011) Hallmarks of cancer: the next generation. Cell 144: 646–674. - PubMed
-
- Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, et al. (2006) Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science 313: 1960–1964. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
