

Challenges in detecting HIV persistence during potentially curative interventions: a study of the Berlin patient
- PMID: 23671416
- PMCID: PMC3649997
- DOI: 10.1371/journal.ppat.1003347
Challenges in detecting HIV persistence during potentially curative interventions: a study of the Berlin patient
Abstract
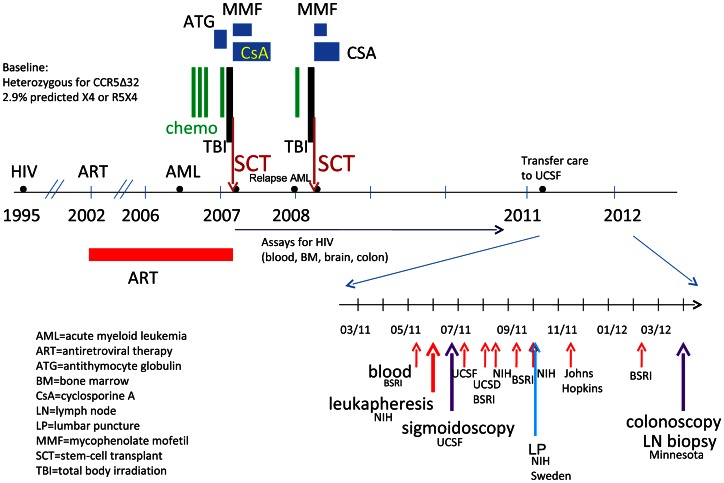
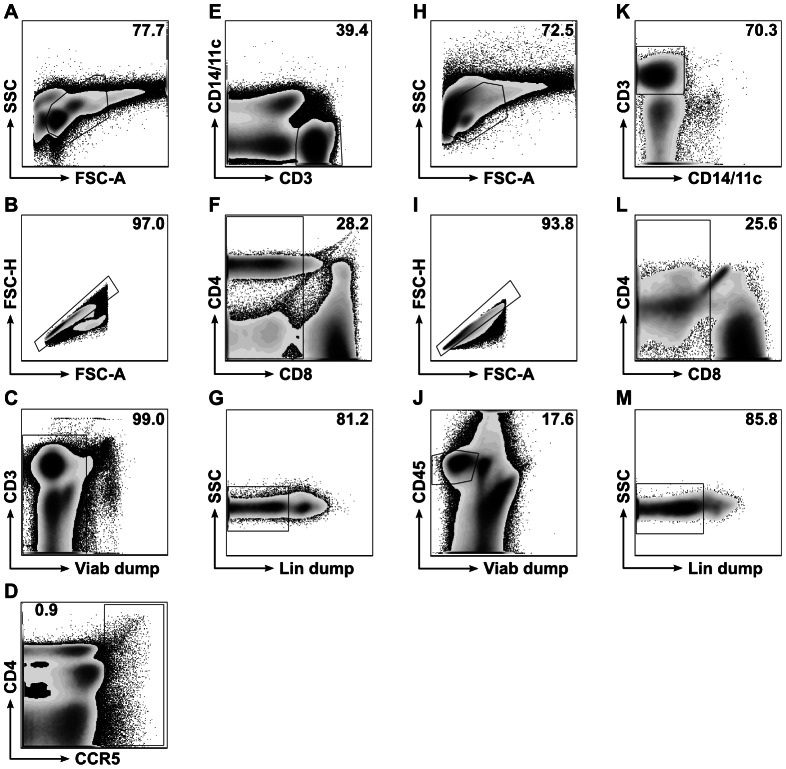
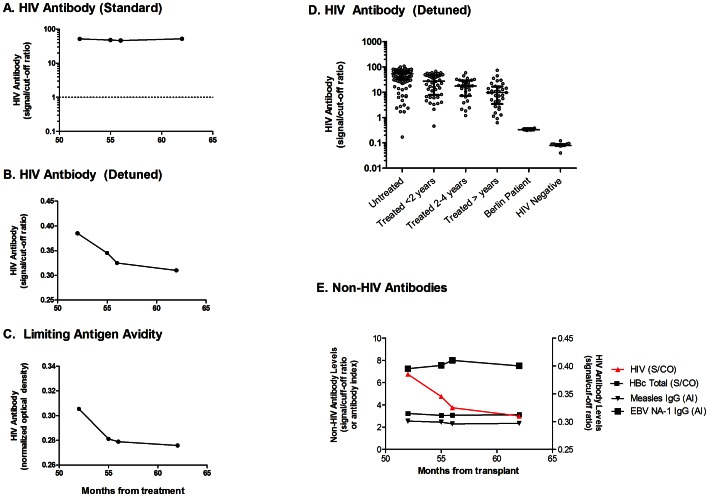
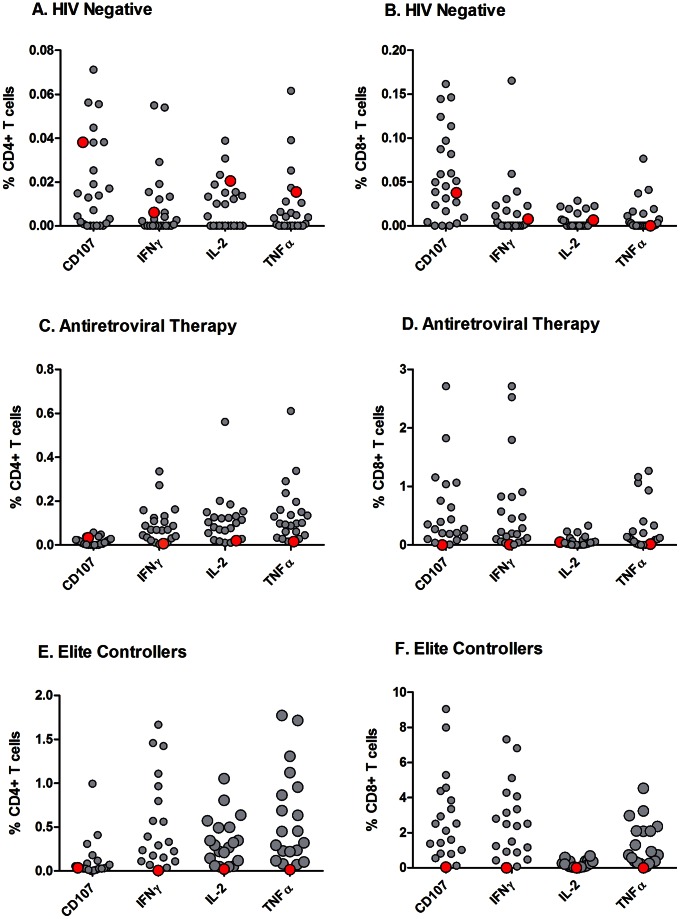
There is intense interest in developing curative interventions for HIV. How such a cure will be quantified and defined is not known. We applied a series of measurements of HIV persistence to the study of an HIV-infected adult who has exhibited evidence of cure after allogeneic hematopoietic stem cell transplant from a homozygous CCR5Δ32 donor. Samples from blood, spinal fluid, lymph node, and gut were analyzed in multiple laboratories using different approaches. No HIV DNA or RNA was detected in peripheral blood mononuclear cells (PBMC), spinal fluid, lymph node, or terminal ileum, and no replication-competent virus could be cultured from PBMCs. However, HIV RNA was detected in plasma (2 laboratories) and HIV DNA was detected in the rectum (1 laboratory) at levels considerably lower than those expected in ART-suppressed patients. It was not possible to obtain sequence data from plasma or gut, while an X4 sequence from PBMC did not match the pre-transplant sequence. HIV antibody levels were readily detectable but declined over time; T cell responses were largely absent. The occasional, low-level PCR signals raise the possibility that some HIV nucleic acid might persist, although they could also be false positives. Since HIV levels in well-treated individuals are near the limits of detection of current assays, more sensitive assays need to be developed and validated. The absence of recrudescent HIV replication and waning HIV-specific immune responses five years after withdrawal of treatment provide proof of a clinical cure.
Conflict of interest statement
Michael Busch has consulted for Gen-Probe (now owned by Hologic), which provided support for some of the virologic measurements performed in this study. Christopher Bentsen is currently employed by Bio-Rad Laboratories, Inc. and received salary, benefits and stock. He oversaw the testing of samples in this paper with FDA approved tests from Bio-Rad. These relationships do not alter our adherence to all PLoS Pathogens policies on sharing data and materials.
Figures
Similar articles
-
Evidence for HIV-1 cure after CCR5Δ32/Δ32 allogeneic haemopoietic stem-cell transplantation 30 months post analytical treatment interruption: a case report.Lancet HIV. 2020 May;7(5):e340-e347. doi: 10.1016/S2352-3018(20)30069-2. Epub 2020 Mar 10. Lancet HIV. 2020. PMID: 32169158 Free PMC article.
-
Mechanisms That Contribute to a Profound Reduction of the HIV-1 Reservoir After Allogeneic Stem Cell Transplant.Ann Intern Med. 2018 Nov 20;169(10):674-683. doi: 10.7326/M18-0759. Epub 2018 Oct 16. Ann Intern Med. 2018. PMID: 30326031
-
Comparative Analysis of Cell-Associated HIV DNA Levels in Cerebrospinal Fluid and Peripheral Blood by Droplet Digital PCR.PLoS One. 2015 Oct 2;10(10):e0139510. doi: 10.1371/journal.pone.0139510. eCollection 2015. PLoS One. 2015. PMID: 26431315 Free PMC article.
-
Hematopoietic stem cell transplantation for HIV cure.J Clin Invest. 2016 Feb;126(2):432-7. doi: 10.1172/JCI80563. Epub 2016 Jan 5. J Clin Invest. 2016. PMID: 26731468 Free PMC article. Review.
-
Lessons Learned From Failures and Success Stories of HIV Breakthroughs: Are We Getting Closer to an HIV Cure?Front Microbiol. 2020 Jan 31;11:46. doi: 10.3389/fmicb.2020.00046. eCollection 2020. Front Microbiol. 2020. PMID: 32082282 Free PMC article. Review.
Cited by
-
Intradermal injection of a Tat Oyi-based therapeutic HIV vaccine reduces of 1.5 log copies/mL the HIV RNA rebound median and no HIV DNA rebound following cART interruption in a phase I/II randomized controlled clinical trial.Retrovirology. 2016 Apr 1;13:21. doi: 10.1186/s12977-016-0251-3. Retrovirology. 2016. PMID: 27036656 Free PMC article. Clinical Trial.
-
Why and where an HIV cure is needed and how it might be achieved.Nature. 2019 Dec;576(7787):397-405. doi: 10.1038/s41586-019-1841-8. Epub 2019 Dec 18. Nature. 2019. PMID: 31853080 Free PMC article. Review.
-
Novel small synthetic HIV-1 V3 crown variants: CCR5 targeting ligands.J Biochem. 2022 Sep 5;172(3):149-164. doi: 10.1093/jb/mvac052. J Biochem. 2022. PMID: 35708645 Free PMC article.
-
Second example reported of a stem-cell transplant in the clinic leading to HIV remission.Nature. 2019 Apr;568(7751):175-176. doi: 10.1038/d41586-019-00989-y. Nature. 2019. PMID: 30962552 No abstract available.
-
CCR5 as a natural and modulated target for inhibition of HIV.Viruses. 2013 Dec 30;6(1):54-68. doi: 10.3390/v6010054. Viruses. 2013. PMID: 24381033 Free PMC article.
References
-
- Richman DD, Margolis DM, Delaney M, Greene WC, Hazuda D, et al. (2009) The challenge of finding a cure for HIV infection. Science 323: 1304–1307. - PubMed
-
- Hutter G, Nowak D, Mossner M, Ganepola S, Mussig A, et al. (2009) Long-term control of HIV by CCR5 Delta32/Delta32 stem-cell transplantation. The New England journal of medicine 360: 692–698. - PubMed
-
- Allers K, Hutter G, Hofmann J, Loddenkemper C, Rieger K, et al. (2011) Evidence for the cure of HIV infection by CCR5Delta32/Delta32 stem cell transplantation. Blood 117: 2791–2799. - PubMed
-
- Symons J, Deeks S, Hutter G, Wensing A, Martin J, et al... (2012) The cure of the ‘Berlin patient’: why did pre-existing X4-variants not emergence after allogeneic CCR5-Δ32 SCT?. 19th International AIDS Conference. Washington, D.C.
Publication types
MeSH terms
Substances
Grants and funding
- P01 AI080193/AI/NIAID NIH HHS/United States
- IK2 CX000520/CX/CSRD VA/United States
- R01 AI047745/AI/NIAID NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- K24 AI069994/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- P01 AI074340/AI/NIAID NIH HHS/United States
- U19 AI096113/AI/NIAID NIH HHS/United States
- R24 AI106039/AI/NIAID NIH HHS/United States
- 1 IK2 CX000520-01/CX/CSRD VA/United States
- P01 AI071713/AI/NIAID NIH HHS/United States
- U19 AI096109/AI/NIAID NIH HHS/United States
- AI047745/AI/NIAID NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- R21 AI047745/AI/NIAID NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- AI74621/AI/NIAID NIH HHS/United States
- R21 MH096619/MH/NIMH NIH HHS/United States
- AI306214/AI/NIAID NIH HHS/United States
- R01 AI087145/AI/NIAID NIH HHS/United States
- R56 AI047745/AI/NIAID NIH HHS/United States
- U19AI0961090/AI/NIAID NIH HHS/United States
- AI69432/AI/NIAID NIH HHS/United States
- P01 AI074621/AI/NIAID NIH HHS/United States
- AI 080193/AI/NIAID NIH HHS/United States
- AI096113/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
