

Underestimation of liver-related mortality in the United States
- PMID: 23583430
- PMCID: PMC3890240
- DOI: 10.1053/j.gastro.2013.04.005
Underestimation of liver-related mortality in the United States
Abstract
Background & aims: According to the National Center for Health Statistics (NCHS), chronic liver disease and cirrhosis is the 12(th) leading cause of death in the United States. However, this single descriptor might not adequately enumerate all deaths from liver disease. The aim of our study was to update data on liver mortality in the United States.
Methods: Mortality data were obtained from the Rochester Epidemiology Project (1999-2008) and the National Death Registry (1979-2008). Liver-specific mortality values were calculated. In contrast to the narrow NCHS definition, updated liver-related causes of death included other specific liver diagnoses (eg, hepatorenal syndrome), viral hepatitis, and hepatobiliary cancers.
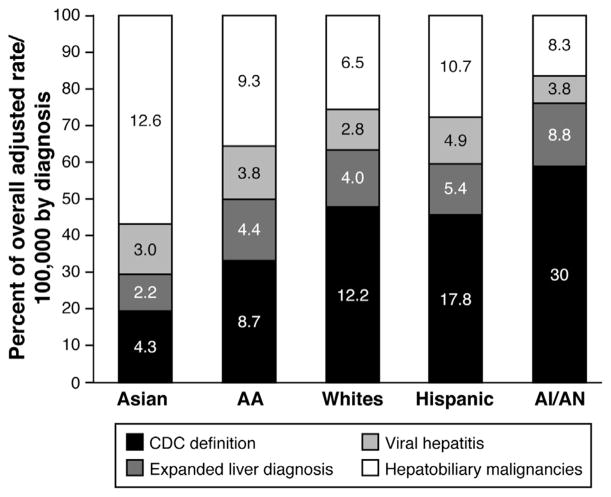
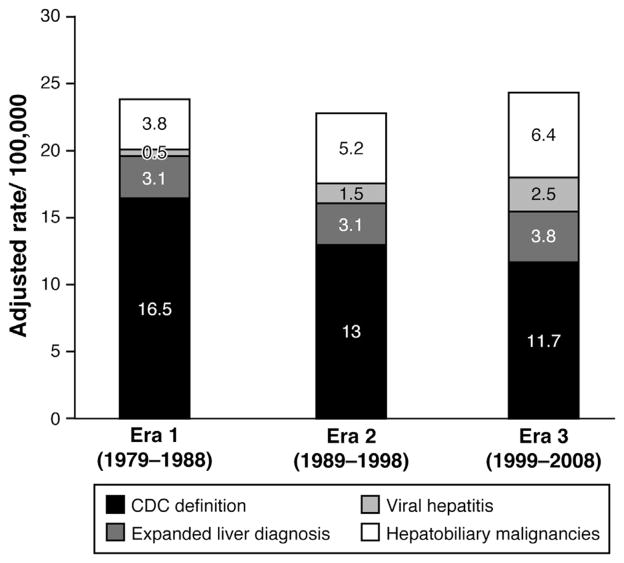
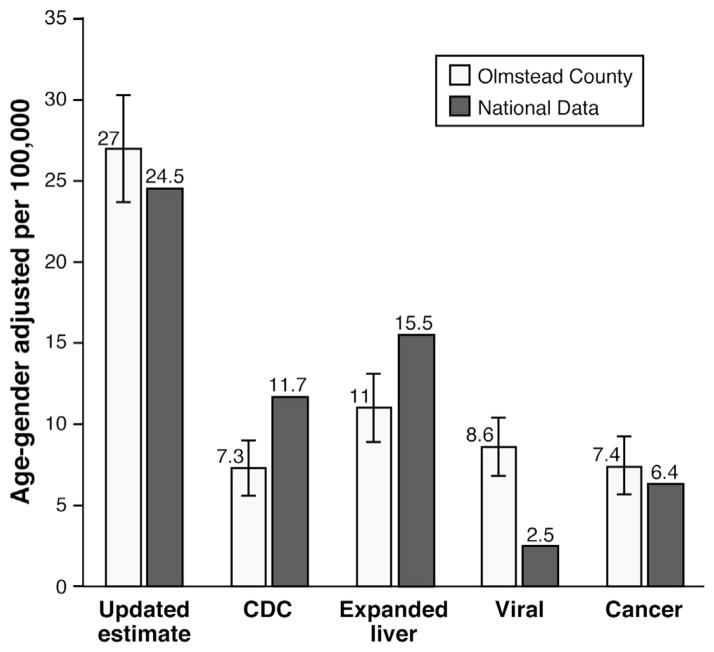
Results: The Rochester Epidemiology Project database contained information on 261 liver-related deaths, with an age- and sex-adjusted death rate of 27.0/100,000 persons (95% confidence interval: 23.7-30.3). Of these, only 71 deaths (27.2%) would have been captured by the NCHS definition. Of cases for which viral hepatitis or hepatobiliary cancer was the cause of death, 96.9% and 94.3% had liver-related immediate causes of death, respectively. In analysis of data from the National Death registry (2008), use of the updated definition increased liver mortality by >2-fold (from 11.7 to 25.7 deaths/100,000, respectively). Using NCHS definitions, liver-related deaths decreased from 18.9/100,000 in 1979 to 11.7/100,000 in 2008-a reduction of 38%. However, using the updated estimate, liver-related deaths were essentially unchanged from 1979 (25.8/100,000) to 2008 (25.7/100,000). Mortality burden was systematically underestimated among non-whites and persons of Hispanic ethnicity.
Conclusions: Based on analyses of the Rochester Epidemiology Project and National Death databases, liver-related mortality has been underestimated during the past 2 decades in the United States.
Keywords: CDC; CI; Centers for Disease Control and Prevention; HBV; HCC; HCV; Hepatocellular Carcinoma; ICD; International Classification of Diseases; NCHS; National Center for Health Statistics; Population; REP; Rate of Death; Rochester Epidemiology Project; confidence interval; hepatitis C virus; hepatocellular carcinoma.
Copyright © 2013 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
The authors disclose no conflicts.
Figures

Similar articles
-
Annual Report to the Nation on the Status of Cancer, 1975-2012, featuring the increasing incidence of liver cancer.Cancer. 2016 May 1;122(9):1312-37. doi: 10.1002/cncr.29936. Epub 2016 Mar 9. Cancer. 2016. PMID: 26959385 Free PMC article.
-
Changes in mortality due to Chronic Liver Diseases (CLD) during the COVID-19 pandemic: Data from the United States' National Vital Statistics System.PLoS One. 2024 Sep 3;19(9):e0289202. doi: 10.1371/journal.pone.0289202. eCollection 2024. PLoS One. 2024. PMID: 39226267 Free PMC article.
-
Causes of death in patients with hepatitis B: a natural history cohort study in the United States.Hepatology. 2013 Jul;58(1):21-30. doi: 10.1002/hep.26110. Epub 2012 Dec 12. Hepatology. 2013. PMID: 23080403
-
Hepatitis C and hepatitis B-related mortality in Spain.Eur J Gastroenterol Hepatol. 2009 Aug;21(8):895-901. doi: 10.1097/MEG.0b013e328313139d. Eur J Gastroenterol Hepatol. 2009. PMID: 19357523 Review.
-
Status quo of chronic liver diseases, including hepatocellular carcinoma, in Mongolia.Korean J Intern Med. 2012 Jun;27(2):121-7. doi: 10.3904/kjim.2012.27.2.121. Epub 2012 May 31. Korean J Intern Med. 2012. PMID: 22707881 Free PMC article. Review.
Cited by
-
Outcomes associated with a mandatory gastroenterology consultation to improve the quality of care of patients hospitalized with decompensated cirrhosis.J Hosp Med. 2015 Apr;10(4):236-41. doi: 10.1002/jhm.2314. Epub 2014 Dec 30. J Hosp Med. 2015. PMID: 25557938 Free PMC article.
-
Changes in liver-related mortality by etiology and sequelae: underlying versus multiple causes of death.Popul Health Metr. 2021 Apr 29;19(1):22. doi: 10.1186/s12963-021-00249-0. Popul Health Metr. 2021. PMID: 33926463 Free PMC article.
-
Contemporary Epidemiology of Chronic Liver Disease and Cirrhosis.Clin Gastroenterol Hepatol. 2020 Nov;18(12):2650-2666. doi: 10.1016/j.cgh.2019.07.060. Epub 2019 Aug 8. Clin Gastroenterol Hepatol. 2020. PMID: 31401364 Free PMC article. Review.
-
Hyperoside as a Potential Natural Product Targeting Oxidative Stress in Liver Diseases.Antioxidants (Basel). 2022 Jul 25;11(8):1437. doi: 10.3390/antiox11081437. Antioxidants (Basel). 2022. PMID: 35892639 Free PMC article. Review.
-
Alcohol Consumption and Chronic Liver Disease Mortality in New Mexico and the United States, 1999-2013.Public Health Rep. 2018 May/Jun;133(3):287-293. doi: 10.1177/0033354918766890. Epub 2018 Apr 17. Public Health Rep. 2018. PMID: 29664698 Free PMC article.
References
-
- Heron M. Deaths: Leading causes for 2009. National Vital Statistics Reports. 2012 Oct 26;61(7) - PubMed
-
- Kim WR, Brown RS, Jr, Terrault NA, et al. Burden of liver disease in the United States: summary of a workshop. Hepatology. 2002;36:227–242. - PubMed
-
- Manos MM, Leyden WA, Murphy RC, et al. Limitations of conventionally derived chronic liver disease mortality rates: results of a comprehensive assessment. Hepatology. 2008;47:1150–1157. - PubMed
-
- Davis GL, Alter MJ, El-Serag H, et al. Aging of hepatitis C virus (HCV)-infected persons in the United States: a multiple cohort model of HCV prevalence and disease progression. Gastroenterology. 2010;138:513–521. 521 e1–e6. - PubMed
-
- Mitchell AE, Colvin HM, Palmer Beasley R. Institute of Medicine recommendations for the prevention and control of hepatitis B and C. Hepatology. 51:729–733. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
